
1. Scoop Health: Review of Cannabis by the World Health Organisation
World Health Organisation’s 40th Expert Committee on drug dependence (ECDD) reviewing Cannabis.
This week marks a historic turning point for cannabis as the World Health Organisation’s ECDD conducts its first ever review of the scheduling of cannabis.
Both as a flower and is a concentrated resin.
This has never been done before and in fact the scheduling and the single Convention from 1961 was based on assumptions from earlier international treaties, which were not evidence based.
It is the hope of MCANZ that this review will recommend the change in schedule for cannabis flower and resin and in fact take a more granular approach to cannabis products in general between those that do have some risk of dependence or abuse versus those which have none.
To this end MCANZ has submitted a video submission for the open session which will be presented in Geneva Switzerland.
Of the 12 submissions New Zealand is over-represented with both MCANZ and the Hemp Foundation both submitting, due to the unique nature of its timing with the ongoing political process for law reform in New Zealand.
“It is our hope that with the World Health Organisation review would recommending descheduling, and that perhaps our government could use such recommendations to open up access to less refined and more affordable products”.
“It is a privilege to be selected from the various organisations in the public domain worldwide to present to the WHO on this matter”
“Our hope would be that via the scheduling and the UN single Convention of narcotics 1961 that cannabis products are scheduled in a more granular fashion so that the high CBD products are recognised globally as having no risk and therefore schedule differently, it would require a different methodology similar to what is applied to codeine as even high CBD products have a measurable amount of THC in them.”
“It could be argued that nutmeg, a banned psychoactive substance in Saudi Arabia, has more abuse potential than a high CBD product such as Charlotte’s Web or Haleigh’s Hope for example, yet as a tincture or oil, it is schedule 1, the same status as Oxycodone aka “Hillbilly heroin” ” says MCANZ coordinator Shane Le Brun.
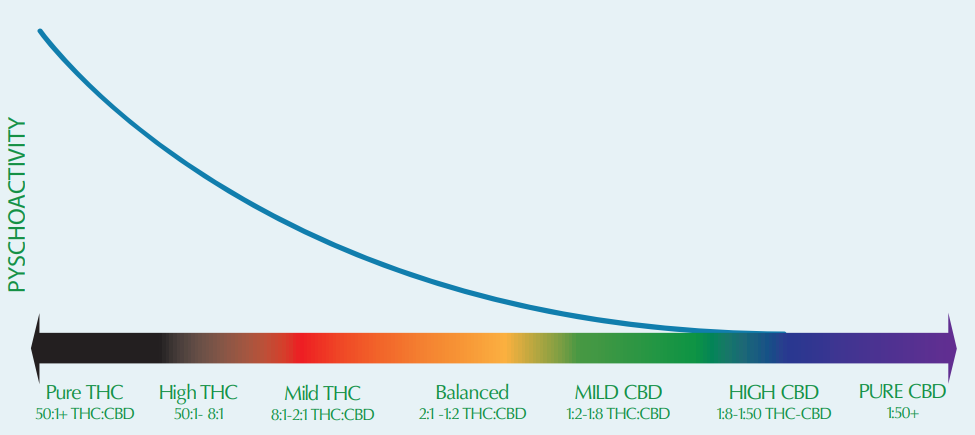
MCANZ refers to its resources at www.mc2018.co.nz for a visual indication on the sliding scale of THC potency vs psychoactivity, (image attached below)
2. Australia21: WHAT IF POLICE STOPPED ARRESTING PEOPLE FOR DRUG USE? FIRST HAND ACCOUNT
In the late 1990s, the increasing use of heroin landed Portugal with a drug-related public health emergency, so the government established an expert advisory board to work out what to do.
The experts advised it to make a major change: deal with people who use drugs through the health system, not the criminal system.
Portugal’s emphasis on treatment instead of punishment has been a major success, providing other governments around the world with a model for more effective laws that reduce both direct and indirect drug harms.
SICAD’s Institutional Values are at the heart of its success: humanism, knowledge, innovation, pragmatism, cooperation, confidence and transparency.
One of the people responsible for putting a stop to criminal convictions and implementing Portugal’s world-leading drug policy is Dr Manuel Cardoso, who’s now Deputy General-Director of the country’s General-Directorate for Intervention on Addictive Behaviours and Dependencies (SICAD).
Dr Cardoso is visiting Australia in June.
While here, he’ll speak at an Unharm and Uniting public forum along with Dr Marianne Jauncey, the medical director of the Sydney Medically Supervised Injecting Centre (MSIC).
The centre opened in 2001 — the same year that drug use was decriminialised in Portgual — and it’s still the only place in New South Wales where possession of a personal quantity of drugs is not a crime.
Dr Jauncey will also share her firsthand experience of what’s possible in a setting where drug use is not criminalised.
They’ll be joined by former Premier of Western Australia Dr. Geoff Gallop, an Advocate for Harm Reduction Australia.
 Dr Cardoso will also deliver the keynote address at the 2018 Conference of NADA, the Network of Alcohol and Other Drug Agencies in NSW.
Dr Cardoso will also deliver the keynote address at the 2018 Conference of NADA, the Network of Alcohol and Other Drug Agencies in NSW.
Here’s a snapshot of an interview conducted ahead of the conference, by NADA’s Clinical Director Dr Suzie Hudson.
A conversation with Manuel Cardoso: drug use, health and human rights
Dr Suzie Hudson: Can you describe the changes that have occurred in Portugal regarding the possession and use of illicit drugs?
Dr Manuel Cardoso: In the eyes of the law before 2000, consumption of drugs was a crime – you could go to prison. Then parliament changed this from a criminal offence to an administrative one.
So the consumption, acquisition and possession for personal use of banned substances was no longer a crime.
It’s only an administrative offence.
The offender is send to a Dissuasion Commission which evaluates the consumption risk and what to do next.
The answer may be treatment, or not.
SH: By taking it away from the criminal system and putting it more centrally in the health system, what had to change then in terms of responding, for those people who perhaps might identify as being concerned about their drug use?
MC: Not so much because before this law, we already determined how many units of treatment we needed: treatment centres, therapeutic communities, and how many places within each.
What is different is the way you look at the issue.
What really changed was the way the person who needed treatment faces the treatment programs.
Most used to be afraid of entering into these kind of programs, as they feared referral to the criminal justice system.
When consuming drugs was a criminal offence, people who helped consumers in any way, for instance with needle exchanges, were also committing a criminal offence.
People who used drugs were labelled ‘criminal’ and therefore were stigmatised, so the people who work with them were stigmatised by association. In this way, things have changed a lot.
Also before, we couldn’t identify people by their real name because they were afraid that the police would identify them at the centres.
Now we can attach the treatment processes to each person–we found more than 20 per cent were duplicate or triplicate.
Now we can treat people using their real name, from one centre to another, nationally.
SH: What would you say was the catalyst, or what were some of the things that led to the change in laws?
MC: So many issues related to this.
Firstly, there was the problem itself.
Remember when we say one per cent of the population had a problematic drug use, it’s a lot of people.
We also know that drug use reaches everyone–every family has someone–and they think…my son, my daughter, is not a criminal.
This is what the population was feeling.
Then the former president of the Republic said something along these lines: I am concerned with all citizens and their problems.
That includes people who use drugs.
Our president promoted many meetings to discuss the issues, and then the government created a Commission composed both by leading public officers and researchers in the field of drugs.
The government asked the commission to prepare a report on how to deal with drug use issues with only one request: don’t go against United Nations conventions.
So, many things moved at the same time to create an atmosphere for change.
We chose decriminalisation and not the legalisation.
The commission proposed decriminalisation and they also proposed prevention and treatment: it’s a comprehensive strategy related to demand and supply.
The main principles of our strategy were humanism and pragmatism.
SH: Are there then people who continue to disagree with the change, I’m wondering?
MC: No. The conservative parties were more strongly opposed to decriminalisation.
However, at the end of 2001, the government changed from socialist party to a conservative one and that conservative government continued the decriminalisation process approved in 2000, and put into place in 2001.
So things have been maintained.
SH: You have mentioned the impact of the changes in the laws as including destigmatisation, access to treatment, and the positive impact on workers in the field. What do you feel like have been some of the major challenges for you and the treatment sector?
MC: The first major challenge was to give treatment to all who asked for it.
I prepared a report to identify how many people we have in treatment, then how many are waiting for an answer or an appointment.
Mid-1998 we had 2,500 people requesting for treatment and not receiving help.
In six months, we reduced this to 600, and one year later all people had treatment if they asked for it.
The second challenge was to help people who didn’t have the ability to seek treatment.
We went to the streets to find those who needed help.
I think this was very interesting and challenging, but it’s in the process to start building a structure of integrated responses.
Then in 2002, we put all the national co-ordination, treatment issues, harm reduction, prevention, re-integration all in the same Institute, in the Health Ministry.
It was challenging to put these people working together in a multi-disciplinary area.
We prepared the ‘National plan against drug and drug addiction’ which was approved by the government.
After that we created a national plan of integrated responses.
But first we had to identify what is the important things to do in small territories–you have to invite the people and those responsible for these small areas to identify problems and the way to solve them.
There are many challenges, trying to harmonise the work in each region is one: it’s different and it’s autonomous.
Now they work together and do things in the same way.
Since 2008 we have become responsible for alcohol issues too.
More than 1,000 people are working on this.
And since 2012, we became responsible for all addictions: gambling, the internet and more.
That’s why we are called Addictive behaviours and dependencies’.
We have no responsibility for tobacco nowadays–in that field, things are working pretty well.
SH: Pharmaceutical drugs?
MC: This is a challenge.
We have lots of people consuming prescribed medicines, a few non prescribed one.
And we have others challenges… but to identify people who drink, who drink a lot, we need to identify this as early as possible.
But people don’t know that they could be having a risk consumption.
We all know that people use–illicit or licit–substances because one of two reasons: in search of pleasure or to relieve pain.
The problem arises when the only way to get pleasure is by using substances.
People drink because they like it, they feel well, they feel good, and in a wine producer country almost everyone drinks.
SH: Yes, it’s very socially acceptable.
MC: For events, or even because you are tired and you need to relax a little.
So, it’s difficult but the idea is to get the primary healthcare (GPs) to ask three questions and then refer those with a problem to our network.
SH: There’s lots of harmony between these experiences you’re describing and what the challenges that we face here and the things that we are doing as well. I think when you come to Australia, there’s lots that we can learn from you and your experiences.
To attend the FREE Unharm and Uniting public forum in Sydney on Tuesday 5 June 2018 click here.
3. CannabisTech: Chromatography – A Badge Of Integrity
As the demand for cannabinoid products continues to climb, businesses are emerging to accommodate this need, some of which are more reputable than others.
Utilizing technology, like chromatography, can help separate quality cannabis and hemp producers from the crowd.
At present, a discrepancy exists between federal and state laws, so there are no nationally standardized regulations for hemp and cannabis supplements.
While all products should be tested for composition, content, potency, adulterants and toxic residues, many times quality control is lacking.
Without standardization, it is difficult for consumers to know who to trust and bad business practices are giving good businesses a black eye.
.jpg)
Using Chromatography To Test For Potency
Different strains of the cannabis plant contain varying levels of active compounds. Diverse environmental conditions can even produce different cannabinoid concentrations within various plants of the same strain.
The fact that cannabis comes from a plant and is not a chemically derived substance makes it difficult to determine content levels and dosage.
Chromatography can help producers and manufacturers deliver a quality, accurately dosed product.
According to a recent paper, Labeling Accuracy of Cannabidiol Extracts Sold Online, the labeling on many CBD products is inaccurate.
The team who contributed to this paper purchased 84 products with labels stating they contained CBD. These samples came from 31 companies and included tinctures, vaporization liquids, and oils.
Testing was performed with high-performance liquid chromatography (HPLC).
Chromatography separates cannabinoids from cannabis and hemp extracts at a molecular level.
One of the big advantages of chromatography is the ability to work with low concentrations and very small samples.

In the legal CBD trade, collected samples revealed only 31% were accurately labeled, and other products contained more or less CBD than stated on the label.
The team also found, out of the 84 samples tested, unreported THC was present in 18 of them.
Using Chromatography To Test For Contaminants
In addition to ensuring quality dosing, chromatography is also being used to test for and remove residual solvents and contaminants.
Pesticides, herbicides, fungicides, and other chemicals used in cultivation can be transferred into the extracts from the plant.
Screening for these types of toxins in extracts intended for human consumption should be fundamental.
In Colorado, the State issues a list of acceptable levels of particular contaminants (section R712) each year.
Due to the efforts of legalization, state regulation helps ensure a safe product for consumers.
However, hemp from a plethora of sources is being utilized to produce cannabidiol supplements for all states.
The hemp could be being produced as “industrial hemp” with less agricultural standards, or it may be imported from foreign sources.
Chromatography: A Badge Of Integrity
The growing popularity of CBD in the health supplement sector and the lack of regulation is the perfect environment for shady business practices.
In a market without federal regulation from the FDA, many cannabis and hemp extracts have less regulation than a candy bar, as pointed out in a press release by Marcel Bonn-Miller, Ph.D. and leading author on the study,
“The big problem, with this being something that is not federally legal, is that the needed quality assurance oversight from the Food and Drug Administration is not available.
There are currently no standards for producing, testing, or labeling these oils.
So, right now, if you buy a Hershey bar, you know it has been checked over; you know how many calories are in it, you know it has chocolate as an ingredient, you know how much chocolate is in there.
Selling these oils without oversight, there is no way to know what is actually in the bottle.
It’s crazy to have less oversight and information about a product being widely used for medicinal purposes, especially in very ill children, than a Hershey bar.”
In states with legal marijuana, strict regulations and rigorous testing are required on all hemp products.
In addition, high-quality crops are organically grown and harvested with state-of-the-art equipment.
Products are tested using cutting-edge technology in laboratories and standardized to contain a specific cannabinoids content.
However, others only see a “get-rich-quick” opportunity, cashing in on the growing demand without concern for the quality of the product or the well-being of the consumer.
Until standards and regulations are officially put in place consumers must rely on the integrity of upstanding business practices.
Utilizing chromatography to ensure a quality product can lead canna-businesses to success.