
1. Robert Kennedy’s World Mercury Project: Yeast in Vaccines Tied to Autoimmune Diseases
It’s well-recognized that the incidence of autoimmune diseases has been rising at an enormous rate.
A study indicates that a significant factor in causing them may be the common bakers or brewers yeast, Sacccharomyces cerevisiae[1] used in many vaccinations, including HepB, which is given to nearly all newborn babies in the United States before they’re a day old.
The specific part of S. cerevisiae that’s of concern is mannan, which is found in the cell walls of yeasts and also in mammalian glycoproteins.
These glycoproteins are found in cell walls, connective tissues like collagen, gastrointestinal mucous secretions, and blood plasma.
They perform many functions.
Obviously, if the immune system goes on the attack against mannan, it can be devastating.
Yet, that appears to be happening in many autoimmune diseases.

These diseases happen when the body’s own defense system turns on itself, resulting in life-eroding conditions like rheumatoid arthritis, Crohn’s disease, inflammatory bowel disease, systemic lupus erythematosus, anti-phospholipid syndrome, multiple sclerosis, diabetes mellitus type 1, and even heart disease.
Both the Centers for Disease Control (CDC) and the National Institutes of Health (NIH) are aware of the increase in autoimmune diseases[2] .
Autoimmune disease research is now included in chapter 3 of the NIH Biennial Report[3] which discusses their approach to dealing with the issue, including the type of research they’re supporting.
Nowhere is there any indication that vaccinations are being considered as a potential cause.
Of course, if you don’t look for it, you are not likely to find it.
Clearly, they are not promoting a genuine investigation into finding the causes of autoimmune disorders, as they’re willing to consider anything and everything … except the elephant in the room named vaccination.
As is the case with autism, the primary focus is on genetics, with environment also considered—as long as the term environment doesn’t include vaccines.
As with autism, that focus completely ignores the outright absurdity of blaming genetics for new non-infectious disease phenomena.
How Can Yeast Cause Such Terrible Diseases?
Yeast is, of course, used to make bread rise and create the alcohol in beer.
So how can it suddenly turn into an enemy?
The answer is in how it enters the body, and what enters with it.
The purpose of a vaccine is to create a localized storm in the immune system so that it will respond to a co-injected substance, which may be a weakened microbe or a small bit of a microbe, by creating antibodies to it.
An irritant, called an adjuvant, is what causes the immune system storm, and the microbe is called an antigen.
The catch is that other substances injected with the antigen and adjuvant may also be seen as antigens.
If one of those substances is similar to something that naturally exists in the body, then the immune system may create antibodies to part of its own body, creating an autoimmune disease.
Parts of the mannan in yeast are similar or identical to parts of the human body.
So S. cerevisiae—yeast—used in vaccines has the potential of causing autoimmune disorders.
In fact, S. cerevisiae is used in a variety of ways in vaccines.
It is, when used whole, a potent adjuvant[4].
On top of that, genetic manipulation is now being used on it to create artificial antibodies[4], so S. cerevisiae is becoming more common in vaccines.
Autoantibodies of S. cerevisiae
The researchers who focused on autoimmune aspects of S. cerevisiae (yeast) found significant correlations between yeast’s mannan and known autoimmune antigens in several autoimmune diseases.
They found close and, in some instances, exact matches of the genetic sequences. For example, in the case of rheumatoid arthritis, the percent found to match were:
Rheumatoid arthritis
- Rheumatoid factor: 60%
- Bip/GRP78: 71%
- gp130-RAPS: 80%
- EIF4G1: 88%
- Anti-citrullinated collagen type 2: 100%
Not only were there significant sequence matches with four known rheumatoid arthritis auto-antigens, there was a perfect match with one. In other conditions, they found:
Lupus erythematosus
- SmN: 53%
- SSA (Ro): 60%
- snRNP-SmD3: 64%
- SSB (La): 69%
- U2 snRNP B”: 83%
Heart disease
- P-selectin (protein on surface of blood vessels & platelets): 80%
- Myosin (involved with muscle contraction): 88%
- Intercellular adhesion molecule-1 (inflammatory response molecules): 100%
Anti-phospholipid syndrome
- β2-Glycoprotein-1 precursor: 56%
- Annexin A5: 63%
- Anti-CL/β-2GPI Ig light chain variable region: 73%
AIDs-associated antigens
- Thyroglubulin: 52%
- GAD65: 57%
- Zinc transporter 8: 57%
- Transglutaminase: 60%
- Thyroid peroxidase: 71%
- Soluble liver/pancreas antigen: 80%
- Calprotectin (protein S100-A8): 100%
Sclerosis-associated antigens
- Major centromere autoantigen B: 57%
- RNA polymerase III: 67%
- U3-snRNP fibrillarin: 75%
- U3-snRNP MPP10: 75%
- hU3-55kDA: 86%
- Nucleophosmin B23: 88%
A perfect match with a molecule may not be necessary to result in an autoimmune response, so percentages of less than 100% may not indicate lack of an autoimmune response.
However, the closer the match between a molecule and an antigen, the more likely it is that an autoimmune response will occur.
Although you may not generally think of heart disease as an autoimmune disorder, certain forms of it, such as rheumatic heart disease, are known to be—and as this study seems to indicate, others may be, too.
Vaccine Risks
It should be noted that anti-phospholipid syndrome was originally associated with the tetanus vaccine.
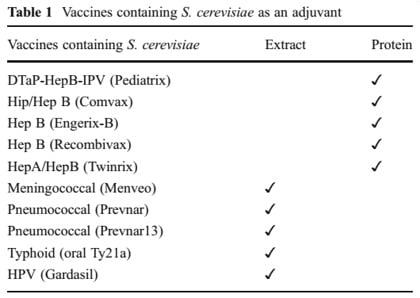
Referring to the table on the right of vaccines containing S. cerevisiae, you can see that the first vaccine listed is DTaP.
The T stands for tetanus.
Do we know for certain that vaccinations containing S. cerevisiae cause these autoimmune diseases?
No, we don’t.
However, we now have information that strongly links yeast-containing vaccines to autoimmune disorders—and we have absolutely nothing to suggest that they don’t cause them.
In fact, not only do we now have the strong association between S. cerevisiae auto-antibodies and mannan-containing proteins, we also have a history of increasing rates of autoimmune disorders that, at a casual look, can be seen to correlate with the expanding vaccination schedules in countries around the world.
Autoimmune disorders are devastating our health and a huge percentage of us suffer from a severely diminished quality of life.
These disorders aren’t happening because of genetic defects, and to suggest that they are is an insult to our intelligence—though that seems to be the goal of our health agencies.
The cost to us as individuals and as a society is enormous.
Surely it’s past time to take a serious and honest look at vaccine risks, including the use of yeast as an ingredient.
Instead, we have a mad rush to create ever-more yeast-related vaccines, because modern recombinant DNA technologies have made it so much easier, faster, and cheaper to produce them.
Unfortunately, though, to step back and apply the precautionary principle isn’t profitable.
So, you can expect to see more and more of them, no matter how much harm they produce.
Sources:
- Anti-Saccharomyces cerevisiae Autoantibodies in Autoimmune Diseases: from Bread Baking to Autoimmunity; Clinical Reviews in Allergies and Immunology;Maurizio Rinaldi, Roberto Perricone, Miri Blank, Carlo Perricone, & Yehuda Shoenfeld; DOI 10.1007/s12016-012-8344-9
- Autoimmune Disease Rates Increasing
- Autoimmune disease research, Chapter 3, NIH Biennial Report.
- Saccharomyces cerevisiae: a versatile eukaryotic system in virology; Microbial Cell Factories; Rui P Galao, Nicoletta Scheller, Isabel Alves-Rodrigues, Tanja Breinig, Andreas Meyerhans and Juana Díez; doi:10.1186/1475-2859-6-32
2. Dr Judy Wilyman Report: Newsletter 195 Vaccines and Medical Freedom in Australia
20 March 2018
In Australia and the US doctors / health practitioners are being required to promote government vaccination policies by their professional regulatory boards.
This is being achieved by choosing the “accepted” literature and by dismissing the serious risks of vaccines as “anti-vaccination“.
The authorities are not allowing scientific debate on the risks and benefits of this medical procedure and health practitioners are not provided with the ingredients of vaccines or their adverse events in their medical education.
Please read the letter below that describes what happens when a medical doctor in the US or Australia assesses the full body of medical lterature on vaccines for themselves.
This letter was sent to ~60 University of Wollongong academics, some of whom are promoting false claims about vaccines on the UOW website that have not been supported by addressing the academic arguments in my PhD thesis on this topic which is also published on the UOW website):
19 March 2018
Copied to UOW Vice-Chancellor Paul Wellings, Professor’s Heather Yeatman and Alison Jones and UOW Academics,
Dear Concerned Australians and Global Community,
I have copied UOW academics into this email because Professor Heather Yeatman has promoted the government’s pro-vaccine claims about immunisation on the UOW website without ever researching the control of infectious diseases in Australia or the ingredients of vaccines and how vaccines are trialled for safety and efficacy.
Her UOW colleagues were asked to sign their names to this promotion in January 2016 also without researching this topic or addressing my in-depth research on this topic.
My research is published on the University of Wollongong website because it is evidence-based.
UOW Vice-Chancellor, Paul Wellings and the UOW academics in this email can remain silent on this topic but they can never say they did not know that they were promoting false information about vaccines to the public that is not evidence-based and will harm human health.
The right to bodily integrity (without coercion for welfare benefits, early childhood education, or employment) for some individuals has already been lost in Australia. This includes children and university students who are doing degrees in health / medicine and some other professions. Now there is a push in Australia for nurses and other professionals to get mandatory flu vaccines.
Please watch this half hour video of a doctor in Ohio who got sick from the flu vaccine and after investigating the ingredients of vaccines (as this is not taught in medical school) he linked them to the escalating chronic illness in the population and publicised this plausible cause of illness in an article. Then he lost his job.
Vaccines a Doctor’s Perspective
I also know of a doctor who had a flu vaccine whilst she was pregnant and her child was born disabled.
This is anecdotal but the story is common and the damage is not systematically monitored or publicised by the Australian government.
This should have been done before the vaccine was approved for all pregnant women – but it was not.
The pharmaceutical companies do not use inert placebos in vaccine trials and there are no independent trials on vaccines.
Here are the ingredients of vaccines taken from the US CDC website. We use many of the same vaccines in Australia but they are licensed under a different name.
I have also provided an information sheet on the flaws in the Maurice-Blackburn lawyers arguments that are being used to justify the removal of vaccination rights in Australia.
Please forward this to your family and friends and fight for your right for medical freedom and bodily integrity that are not being protected in Australia.
Kind regards,
Dr. Judy Wilyman
Bachelor of Science, University of NSW
Diploma of Education (Science), University of Wollongong
Master of Science (Population Health), Faculty of Health Sciences, University of Wollongong.
PhD in The Science and Politics of the Australian Government’s Vaccination Program, UOW School of Social Science, Media and Communication (re-named the School of Humanities and Social Inquiry in 2014).
3. NVIC – Prepare For Change: How Vaccinated Kids Infect The Non-Vaccinated
![]()
With the thousands of mainstream media articles blaming the non-vaccinated for disease outbreaks, this article will provide a necessary counterbalance by showing the vaccinated can (and do) infect the non-vaccinated…
A groundbreaking study published in 2013 in the journal Vaccine titled, “Comparison of virus shedding after lived attenuated and pentavalent reassortant rotavirus vaccine,” referenced the fact that rotavirus vaccines contain live viruses capable of causing infection, shedding and even transmission to non-vaccinated subjects:
“In fact, transmission of these two rotavirus vaccines or vaccine-reassortment strains to unvaccinated contacts has been detected [9–13][1], even in the absence of symptoms.”
One of the five studies referenced in the passage above confirming that the vaccinated can infect the non-vaccinated, “Sibling transmission of vaccine-derived rotavirus (RotaTeq) associated with rotavirus gastroenteritis,” published in 2009, is the first report in the literature to identify the transmission of rotavirus vaccine-derived virus to unvaccinated contacts resulting in symptomatic rotavirus gastroenteritis requiring emergency medical attention:
“We document here the occurrence of vaccine-derived rotavirus (RotaTeq [Merck and Co, Whitehouse Station, NJ]) transmission from a vaccinated infant to an older, unvaccinated sibling, resulting in symptomatic rotavirus gastroenteritis that required emergency department care.”
The study also indicated that two of the five strains of rotavirus within the Rotateq reassorted to produce a more harmful virus either within the vaccinated infant or within the subsequently infected unvaccinated sibling:
“Results of our investigation suggest that reassortment between vaccine component strains of genotypes P7[5]G1 and P1A[8]G6 occurred during replication either in the vaccinated infant or in the older sibling, raising the possibility that this reassortment may have increased the virulence of the vaccine-derived virus.”
This phenomenon of Rotateq vaccine strain reassortment and subsequent gastoenteritis infection in vaccine recipients was also observed in a 2012 study in 61 infants.[2]
Additionally, a Nicaraguan study published in 2012 found “the widespread use of the RotaTeq vaccine has led to the introduction of vaccine genes into circulating human RVs.,” revealing that the widespread introduction of the vaccine strain has altered the genetic makeup of wild-type rotavirus that now infects exposed populations.[3]
It has been estimated that between 80-100% of infants shed rotavirus at some point during 25-28 days after vaccination.[4] [5]
This reveals that the vaccinated, contrary to widespread assumptions about the the risks represented by the non-vaccinated, pose a clear risk of infecting the non-vaccinated, and may be producing the ideal virological conditions for the recombination of diverse rotavirus strains into vaccine-resistant ‘super viruses.’
Another case study, reported on in the National Vaccine Information Center’s document on vaccine viral shedding:
“In 2010, a case report was published in Pediatrics describing a 30-month old healthy boy who had never received rotavirus vaccine and was infected with vaccine strain rotavirus. 237.
He ended up in the emergency room with severe gastroenteritis 10 days after his healthy two-month old brother was given a dose of Merck’s RotaTeq vaccine. A stool sample was taken in the emergency room and came back positive for RotaTeq vaccine derived strains after RT-PCR testing.”
The authors of the case report noted that “transmission of RotaTeq strains to unvaccinated contacts was not evaluated in the pivotal [pre-licensure] clinical trials.” They added that both RotaTeq and Rotarix [GlaxoSmithKline Biologicals] vaccines have “the potential for vaccine-virus transmission to contacts.”
The Rotateq Vaccine: Shot Through with Conflict of Interest
The Rotateq rotavirus vaccine was co-created by Dr. Paul Offit, widely recognized as the vaccine industry’s leading promoter and apologist.
He is the co-patent holder of one of two live rotavirus vaccines the FDA has approved, and which the CDC recommends should be administered to infants in 3 doses at ages 2 months, 4 months, and 6 months.
Historically incapable of self-recusal, despite his glaring conflicts of interest, Offit regularly positions himself as an expert on vaccines, even though he personally gains from presenting his product (and the CDC’s vaccine schedule as a whole) as safe and effective.
Case in point, in one notorious interview in Parenting magazine he claimed a child can receive 10,000 vaccines simultaneously without harm (corrected from 100,000 which he suggested in a previous interview).
The Rotavirus Vaccine Was Dirty from the Start
The first rotavirus vaccine – Rotashield – comprised of four reassorted rhesus-human rotaviruses was approved in 1999, only to be withdrawn from the market by the FDA nine months later when it was found to increase the risk for a deadly form of bowel obstruction known as intussusception in a small subset of highly vulnerable children.[6]
Offit’s Rotateq, which consists of 5 reassorted human-bovine retroviruses (yes, that means GMO), was believed to be a safer alternative when it was approved by the FDA in 2006, but newly published research reveals his vaccine suffers from the same exact deadly problems.
Published this month in Vaccine and titled, “a Intussusception risk after RotaTeq vaccination: Evaluation from worldwide spontaneous reporting data using a self-controlled cse series approach“, the study evaluated worldwide reports to the manufacturer of Rotateq up to May 2014, adjusting for the phenomenon of under-reporting.
The study found that the relative risk of intussception associated with the administration of Rotateq vaccine increases “3-7 days following vaccination, mainly after the first dose and marginally after the second and third doses.”
The increase in relative risk reached 3.45 fold in the period 3-to-7 days after the first dose, relative to the 15-30-day period control period.
Another study linking Rotateq to intussusception was published last year in the New England Journal of Medicine finding approximately 1.5 (95% CI, 0.2 to 3.2) excess cases of intussusception per 100,000 recipients of the first dose.[7]
Live Vaccines: A Pandora’s Box of Adventitious Viruses
Death or debilitation by bowel obstruction rapidly following Rotateq vaccination is an acute adverse effect that is unlikely to be overlooked or ignored.
This is why the Vaccine Adverse Effects Reporting System (VAERS): a passive, vaccine post-marketing surveillance system, has found it to be a significant side effect.
VAERS, however, is believed to capture as little as less than 1% of the actual damage being done by vaccines, indicating that the extent of harm of the Rotateq is several orders of magnitude than presently indicated by this report.
Exposure to Rotateq therefore suffers – like many live vaccines – from a darker side, as far as adverse effects go, which may take months, years, or decades to manifest as part of the multifactorial smog cloud of modern day toxicities and exposures that eventually make their way into the bottleneck of a classical diagnosis.
Rotateq, for instance, has been identified to be contaminated with a number of adventitious viruses; that is to say, viruses that contaminated the live cells and/or biological components involved in the original vaccine manufacturing process. These surreptitious agents, unknown to the manufacturers and regulatory agencies that approved them, infected the vaccines the children given them. These viruses include:
- Porcine Circovirus 1 (PCV-1): In 2010 the FDA suspended the Rotarix vaccine due to the discovery that it was contaminated with PCV-1 virus, a pig virus, the implications of which as far as human exposure are still unknown. Considered less a risk than PCV-2, known to cause a debilitating wasting disease in piglets, the FDA determined, after review, that PCV-1 does not represent a risk to the millions of children exposed to it.
- Porcine Circovirus 2 (PCV-2): A 2014 study conducted by CDC researchers and published in Human Vaccines & Immunotherapeutcs titled, “Detection of PCV-2 DNA in stool samples from infants vaccinated with RotaTeq®,” found for the first time that PCV-2 is shed in the stool of those vaccinated with Rotateq.
They found “A total of 235 (28.5%) samples from 59 vaccine recipients were positive for PCV-2 DNA by one or more assays used in this study.
” Additionally, “Twenty-two of the 102 vaccine recipients (21.6%) shed RotaTeq® vaccine strain and 10 of these vaccinees (9.8%) were shedding both PCV DNA and rotavirus vaccine RNA.”
In pigs, PCV-2 has been linked to serious health problems including, “PCV2-associated pneumonia, PCV2-associated enteritis, PCV2-associated reproductive failure, and Porcine Dermatitis and Nephropathy Syndrome (PDNS).” [source]. In 2010, The FDA ruled, against the precautionary principle, that neither “PCV1 or PCV2 are known to infect or cause illness in humans, however PCV2 may cause illness in pigs.”
- Baboon endogenous strain 7 retrovirus DNA: a 2014 study published inAdvances in Virology titled, “Screening of Viral Pathogens from Pediatric Ileal Tissue Samples after Vaccination,” found evidence of contamination with a baboon retrovirus.
- Class D Simian Retovirus: a 2010 study published in Journal of Virology revealed that the Rotateq vaccine contains simian retrovirus DNA (with a 96% match of certainty), which Judy Mikovits, PhD, confirms may contribute to adverse health effects, regardless of whether it is a self-replicating virus or not.
Because live vaccines are manufactured through co-culturing cells and biological fluids from various different species, there is plenty of opportunity for viruses to adapt to, and recombine to produce infectious agents capable of far greater virulence.
Rotateq is just one of many vaccines in the CDC’s immunization schedule that contain live viruses capable of infecting those given it, including retroviruses, which have been called a modern-day Plague owing to the fact that they are capable of infecting the host as non-HIV acquire immunodeficiency viruses. For more information read Dr. Judy Mikovits and Kent Heckenlively’s new book Plague or listen to my interview of Dr. Mikovits on Fearless Parent Radio.
Clearly, given the evidence revealing the potential unintended, adverse effects of the Rotateq vaccine, especially the potential for it to infect those exposed to it with adventitious viruses, the implementation of the precautionary principle requires the immediate suspension of its use until proper toxicological reevaluations can be made.
Anyone who questions the safety of the present CDC immunization schedule should be able to point to the Rotateq as a perfect example of why the schedule is not at all evidence based but rather founded in a mythological belief in the safety and effectiveness of products that have never been proven sound.
REFERENCES
[1] [9] Phua KB, Quak SH, Lee BW, Emmanuel SC, Goh P, Han HH, et al. Evaluation of RIX4414, a live, attenuated rotavirus vaccine, in a randomized, double-blind, placebo-controlled phase 2 trial involving 2464 Singaporean infants. J Infect Dis 2005;192(Suppl. 1):S6–16.
[10] Dennehy PH, Brady RC, Halperin SA, Ward RL, Alvey JC, Fischer Jr FH, et al. Comparative evaluation of safety and immunogenicity of two dosages of an oral live attenuated human rotavirus vaccine. Pediatr Infect Dis J 2005;24:481–8.
[11] Payne DC, Edwards KM, Bowen MD, Keckley E, Peters J, Esona MD, et al. Sibling transmission of vaccine-derived rotavirus (RotaTeq) associated with rotavirus gastroenteritis. Pediatrics 2010;125:e438–41.
[12] Boom JA, Sahni LC, Payne DC, Gautam R, Lyde F, Mijatovic-Rustempasic S, et al. Symptomatic infection and detection of vaccine and vaccine-reassortant rotavirus strains in 5 children: a case series. J Infect Dis 2012;206:1275–9.
[13] RiveraL,Pen ̃aLM,StainierI,GillardP,CheuvartB,SmolenovI,etal.Horizontal transmission of a human rotavirus vaccine strain—a randomized, placebo- controlled study in twins. Vaccine 2011;29:9508–13.
[2] J Infect Dis. 2012 Aug 1;206(3):377-83. doi: 10.1093/infdis/jis361. Epub 2012 May 21.
Identification of strains of RotaTeq rotavirus vaccine in infants with gastroenteritis following routine vaccination. Donato CM1, Ch’ng LS, Boniface KF, Crawford NW, Buttery JP, Lyon M, Bishop RF, Kirkwood CD.
[3] Infect Genet Evol. 2012 Aug;12(6):1282-94. doi: 10.1016/j.meegid.2012.03.007. Epub 2012 Apr 2.
Vaccine-derived NSP2 segment in rotaviruses from vaccinated children with gastroenteritis in Nicaragua. Bucardo F1, Rippinger CM, Svensson L, Patton JT.
[4] Phua KB, Quak SH, Lee BW, Emmanuel SC, Goh P, Han HH, et al. Evaluation of RIX4414, a live, attenuated rotavirus vaccine, in a randomized, double-blind, placebo-controlled phase 2 trial involving 2464 Singaporean infants. J Infect Dis 2005;192(Suppl. 1):S6–16.
[5] Comparison of virus shedding after lived attenuated and pentavalent reassortant rotavirus vaccine
[6] Centers for Disease Control and Prevention. Intussusception among recipients of rotavirus vaccine—United States, 1998–1999. JAMA 1999;282:520–1 CrossRefMedlineWebof Science
[7] N Engl J Med. 2014 Feb 6;370(6):503-12. doi: 10.1056/NEJMoa1303164. Epub 2014 Jan 14 Intussusception risk after rotavirus vaccination in U.S. infants. Yih WK1, Lieu TA, Kulldorff M, Martin D, McMahill-Walraven CN, Platt R, Selvam N, Selvan M, Lee GM, Nguyen M
One response to “The Safe Vaccine Debate – 1. Robert Kennedy’s World Mercury Project: Yeast in Vaccines Tied to Autoimmune Diseases 2. Dr Judy Wilyman Report: Newsletter #195 Vaccines and Medical Freedom in Australia 3. NVIC – Prepare For Change: How Vaccinated Kids Infect The Non-Vaccinated”
I am overwhelmed by this information. I thank you for your diligence in researching this subject. I am concerned that the freedom of choice is no longer here. I as there are many have not previously been properly informed of this information. I agree that it is in benefit for the Pharmaceutical companies interests to promote vaccinations. How is it possible to get this information out to the public. Furthermore, how do you fight the Pharmaceutical companies and win for the betterment of mankind?