
By Jeremy R. Hammond, Guest Contributor
The US Centers for Disease Control and Prevention (CDC) recommends that everyone aged six months and up, including pregnant women, get an annual flu shot to protect against the influenza virus.
The mainstream media characterize this recommendation as being firmly grounded in science.
The demonstrable truth of the matter, however, is that what the government and media say science says and what science actually tells us are two completely different things.
By deceiving the public about what the science says, the media serve to manufacture consent for public vaccine policy.
A useful illustration of how the media serve this function is a New York Times article published in January and written by Aaron E. Carroll, a professor of pediatrics at Indiana University School of Medicine and regular Times blogger. The article is titled “Why It’s Still Worth Getting a Flu Shot”, and Carroll’s purpose in writing was to persuade his readers that, even though this season’s influenza vaccine was “particularly ineffective”, everyone should still get it.
Details and Deceptions
The argument Carroll presents is that, even in flu seasons like this past one when the vaccine is not well-matched to the predominant circulating strain of the influenza virus, since the vaccine is so extraordinarily safe, it still confers a great benefit to society.
To support his argument, Carroll cites two studies from the prestigious Cochrane collaboration, a global independent organization specializing in meta-analysis that does not accept any industry funding.
(A meta-analysis is a kind of study in which researchers search the literature for relevant studies and review the body of evidence available by combining the results of studies that meet the inclusion criteria.)
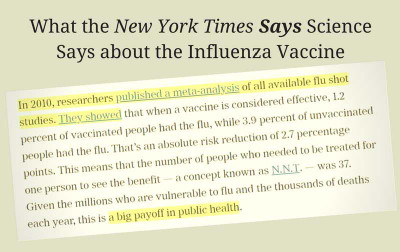 According to Carroll, a 2010 Cochrane review of influenza vaccination in healthy adults found that 37 people need to be vaccinated in order for one person to see the benefit, which represents “a big payoff in public health.”
According to Carroll, a 2010 Cochrane review of influenza vaccination in healthy adults found that 37 people need to be vaccinated in order for one person to see the benefit, which represents “a big payoff in public health.”
Mistakenly describing it as having been published in 2016, Carroll also cites a subsequent 2012 Cochrane review of vaccine effectiveness in healthy children that found “an astonishing payoff in medical terms”: just six children aged six or younger had to be vaccinated in order to prevent one case of influenza.
Carroll further claims that the science shows us that harms from the flu vaccine are “almost nonexistent”.
Carroll could have made his case stronger by citing the actual number from the 2010 Cochrane review, which is 33, not 37.
This was an error Carroll evidently carried over from a secondary source, which is perhaps an indication that he never read the actual Cochrane review, which might also help explain how he could so grossly mischaracterise that review’s actual findings, as you’re about to see.
For starters, it is curious why Carroll would cite the estimated effectiveness of the vaccine “under ideal conditions”—which is to say when the vaccine completely matches the circulating virus—in order to support his argument that it’s worth getting even in poorly matched years.
Why didn’t he instead cite the study’s more relevant estimate of vaccine effectiveness under “average conditions”, when the vaccine only partially matches the circulating strains?
The most obvious answer is that relaying the review’s finding that “100 people need to be vaccinated to avoid one set of influenza symptoms” would be counterproductive to his purpose.
 But that’s just the start of Carroll’s deception.
But that’s just the start of Carroll’s deception.
Whereas he characterizes the 2010 review as though the science fully vindicates public policy, in fact the Cochrane researchers were highly critical of the CDC’s recommendation and challenged the fundamental assumptions underlying it.
They observed that the primary rationales the CDC has offered are that mass vaccination will (1) reduce transmission of the virus and (2) reduce the risk of potentially deadly complications from influenza.
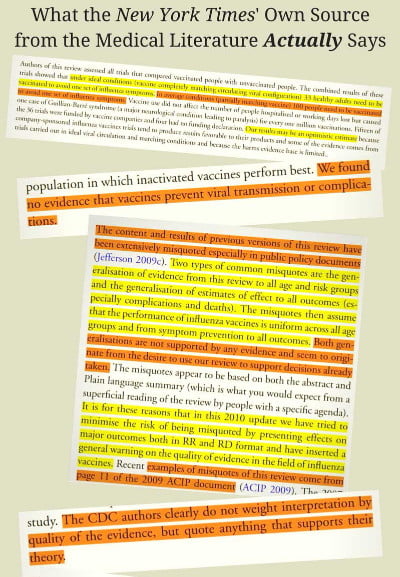
And yet their review turned up “no evidence that vaccines prevent viral transmission or complications” (emphasis added).
In fact, none of the studies they looked at even presented any results “evaluating the ability of this vaccination to interrupt the spread of the disease”. Likewise, none bothered to report “any evidence of effect on complications.”
In other words, none of the studies the Cochrane researchers looked at in their comprehensive review of the literature even seemed to consider the question of whether the central assumptions underlying the CDC’s recommendation were actually true.
This is a remarkable illustration of the institutional myopia that exists when it comes to the politically sensitive issue of vaccines.
Ignoring the Warnings
Once recent study, however, did bother to look at the question of whether the vaccine prevents transmission.
Published on January 18, 2018, in the journal of the Proceedings of the National Academy of Sciences of the United States of America, PNAS, the study’s authors screened volunteers with confirmed cases of influenza and took breath samples.
And among their findings was “an association between repeated vaccination and increased viral aerosol generation” (emphasis added).
In fact, subjects who had received the influenza vaccine in both the current and the previous season were found to shed over six times more aerosolized virus than those who did not get a flu shot during either season.
Another thing Aaron Carroll failed to disclose to Times readers is the rather important caveat that the Cochrane researchers attached to their findings about the vaccine’s effectiveness. And it’s not as though this caveat was easy for him to miss; it’s presented as an explicit “WARNING” right at the top of the review just below the abstract.
The authors’ warning notes that their review included numerous studies funded by the pharmaceutical industry, which independent studies have unsurprisingly shown to be biased in favor of their own products.
The Cochrane researchers found not only that “reliable evidence on influenza vaccines is thin”, but also that “there is evidence of widespread manipulation of conclusions and spurious notoriety of the studies.
The content and conclusions of this review should be interpreted in light of this finding.” (Emphasis added.)
In other words, even the estimate of 100 people needing to be vaccinated for one person to receive a benefit may be overly optimistic.
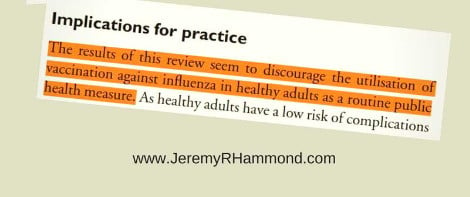
Whereas the Times would have us believe that the Cochrane review found that the flu vaccine confers “a big payoff in public health”, in fact, the conclusion the review authors actually arrived at was that their findings “seem to discourage the utilization of vaccination against influenza in healthy adults as a routine public health measure” (emphasis added).
The Cochrane Collaboration in a 2014 update of their review even more bluntly concluded, “The results of this review provide no evidence for the utilization of vaccination against influenza in healthy adults as a routine public health measure.” (Emphasis added.)
And whereas the Times would have us believe that the science has been settled that harms from the vaccine are “almost nonexistent”, in fact, the 2010 meta-analysis expressed concern about the lack of safety data.
“The harms dataset from randomized studies is small”, they observed, and the studies’ authors “appear to regard harms as less important than effectiveness assessment.”
Even among the studies that weren’t funded by the industry, “the quality of the majority of influenza vaccines studies is low”.
Where’s the Payoff?
Turning to the second Cochrane study Carroll cites, the 2012 review did find that evidence from randomized controlled trials “shows that six children under the age of six need to be vaccinated with live attenuated vaccine to prevent one case of influenza”.
However, they once again cautioned that this finding needs to be interpreted in light of the “evidence of widespread manipulation of conclusions and spurious notoriety of the studies” tending to show favorable results.
While Carroll describes the finding of the vaccine’s effectiveness in children under six as “an astonishing payoff in medical terms”, he does not relay the review’s finding with respect to children aged six or older, which was that 28 children needed to be vaccinated to prevent one case of influenza.
Why not cite this, number, too, to support his case?
After all, this is even fewer than the number needed to vaccinate for healthy adults, which he described as representing a “big payoff”, so why not point to this even bigger payoff?
Perhaps the reason Carroll did not cite this number is that it wouldn’t have actually helped his case at all, since that result was “not significantly more efficacious than placebo.”
In other words, there was no good evidence that the vaccine is effective at preventing influenza in children older than six.
One would think that information, too, would be worth relaying to the public; but, then, that disclosure would not align with his whole purpose for writing, so it is understandable why Carroll would choose not to mention it.
Yet another fact the Times chose not to disclose to readers is that, far from science having established that harms from the vaccine are “almost nonexistent”, the 2012 review found that there was “no usable data” on the safety of the vaccine for children under two.
In other words, according to Carroll’s own source, the flu vaccine has not been properly studied for safety in children aged six months to two years, despite the CDC recommending routine vaccination of children in this age group.
In fact, while the Cochrane researchers had intended to examine the question of safety as well as effectiveness, the absence of good quality data meant that they could not even carry out safety comparisons.
Furthermore, specific influenza vaccines were known to be “associated with serious harms such as narcolepsy and febrile convulsions.”
Especially in light of such known risks, the review authors remarked that “It was surprising to find only one study of inactivated vaccine in children under two years, given current recommendations to vaccinate healthy children from six months of age…. If immunization in children is to be recommended as a public health policy, large-scale studies assessing important outcomes, and directly comparing vaccine types are urgently required.” (Emphasis added.)
In addition to recommending the vaccine for infants as young as six, the CDC also advises pregnant women to get the flu shot, even during their first trimester.
The aforementioned 2014 Cochrane review looked at the science specifically with this recommendation in mind.
And what they found in their systematic review of the literature was that the number of randomized controlled trials assessing the effects of vaccinating pregnant women was zero.
The absence of proper safety studies is also noted right on the package inserts that the manufacturers include in the box with their products. For example, the insert for GlaxoSmithKline’s inactivated influenza vaccine, Fluarix, discloses that “Safety and effectiveness of FLUARIX have not been established in pregnant women or nursing mothers.”
While limited studies have been done on reproductive and developmental toxicity in rats, there are “no adequate and well-controlled studies in pregnant women.” F
urthermore, “caution should be exercised” when vaccinating breastfeeding mothers since “It is not known whether FLUARIX is excreted in human milk.”
Medical practitioners are advised to inform patients “that safety and efficacy have not been established in pregnant women.”
Mercury Menace
The CDC’s recommendation that pregnant women get the flu shot is all the more disturbing given the fact that multi-dose vials of the flu vaccine contain the preservative Thimerosal, which is half ethylmercury by weight. Ethylmercury is a known neurotoxin that can cross the blood-brain barrier and accumulate in the brain.
It can also cross the placental barrier and enter the brain of the developing fetus.
While Thimerosal-free single-dose versions of the vaccine are available, the CDC does not specify in its recommendation to pregnant women that they should opt for this version in order to avoid unnecessarily exposing their fetus to the toxic effects of mercury.
As a review published in the International Journal of Environmental Research and Public Health in December 2017 noted, “there are no safe blood-level values for any of the heavy metals during pregnancy”, particularly since “the placenta is incapable of protecting a human fetus with regards to neurotoxicants or most other heavy metals.”
The review stated that the practice of including known neurotoxins among vaccine ingredients “has to be considered dangerous, irresponsible, and certainly should be ended.”
The authors further commented that the use of mercury as a vaccine ingredient could explain the finding of a CDC-funded study published last September in the journal Vaccine that found an association between the influenza vaccine and spontaneous abortion.
The CDC researchers looked at the 2010-2011 and 2011-2012 flu seasons and found that women who received a flu shot had twice the risk of having a miscarriage within 28 days of receipt than women who did not get the vaccine. Looking just at the 2010-2011 season, vaccinated women had a 3.7 times greater risk of having a spontaneous abortion.
Moreover, since the 2009 Influenza A(H1N1) pandemic, seasonal influenza vaccines have included a varying pandemic H1N1 (or pH1N1) antigen component; and most alarmingly, the CDC researchers found that vaccinated women who had also received a pH1N1-containing influenza vaccine in the prior season had a 7.7 times higher risk of spontaneous abortion.
Toeing the CDC Line
In sum, whereas the New York Times would have us believe the science is settled that the influenza vaccine confers “a big payoff in public health” and carries “almost nonexistent” risk, even its own sources from the medical literature found no scientific evidence to support the CDC’s recommendation and highlighted the alarming lack of good quality safety studies despite the known serious harms associated with the vaccine.
In fact, whereas the New York Times characterizes the 2010 meta-analysis as though it vindicated public policy, the Cochrane researchers actually went so far in their criticism of the agency as to accuse the CDC of deliberately misrepresenting the science in order to support their policy.
Previous versions of their review, they noted, “have been extensively misquoted especially in public policy documents.”
The specific example they presented of how their findings were being deceptively manipulated by public health officials was a 2009 CDC policy document outlining its rationale for universal influenza vaccination.
As the Cochrane researchers stated, “The CDC authors clearly do not weight interpretation by quality of the evidence, but quote anything that supports their theory.”
It is perhaps not too surprising, therefore, that the New York Times would so deceptively mischaracterize the science regarding the effectiveness and safety of the influenza vaccine, given the fact that, by doing so, it was simply following the CDC’s example.
This article is a condensed adaptation of part one of a multi-part exposé on the influenza vaccine. Click here to read the full original essay.
Click here to sign up for the author’s newsletter to stay updated with his work on vaccines and receive his free downloadable report, “5 Horrifying Facts about the FDA Vaccine Approval Process”.
2. AVN: FaceBook taking down pages that question the safety and effectiveness of vaccination
Below is a screenshot of what people see when they try to access the page from within our borders (please excuse the blurry image):


It isn’t just Facebook
As you can see from the video below, taken from a recent BolenReport blog post, the managers and employees at most if not all of the top social media outlets intentionally suppress or outright ban opinions which are in opposition to current government policies.
Shadow banning, outright bans and removal from searches are just some of the dirty tactics used by these censors-for-hire.
What is the solution?
The only language FaceBook, Twitter and the other forums understand is numbers – so let’s take our numbers away from them.
The AVN Team
3. Elizabeth Hart “OverVaccination“: Meningococcal B vaccination – conflicts of interest in vaccination policy
Email for the attention of: Mr Steven Marshall Premier of South Australia
Mr Marshall, since the recent State election, you have been under pressure to implement a meningococcal B vaccination program in South Australia, i.e. Demand for Steven Marshall to fund meningococcal B strain vaccinations program, as reported in The Advertiser newspaper, 20 March 2018.
Heart-rending stories about rare cases of meningococcal B are reported in the media, for example the recent case of Jordan Braddock of Mount Gambier who sadly died after meningococcal B infection.
Troy Bell, the Member of Parliament for Mount Gambier says he hopes “to get all South Australian children immunised against the dangerous B strain rather than waiting for the jab to get on the national program”.[1]
Tony Pasin, the Federal Member of Parliament for Barker, has taken it upon himself to meet with the vaccine’s manufacturer, GlaxoSmithKline, and to push for the Bexsero meningococcal B vaccine to be fast-tracked onto the taxpayer-funded National Immunisation Program Schedule.[2]
However, meningococcal B is a rare disease and mass vaccination is not justifiable.
The vested interests behind the media promotion of meningococcal B cases must be examined, particularly as the meningococcal B vaccine is being hailed as a ‘magic bullet’ to prevent this disease, a claim that is open to question.
Mr Marshall, so far the Bexsero meningococcal B vaccine has been rejected three times by the Pharmaceutical Benefits Advisory Committee due to multiple uncertainties in relation to the clinical effectiveness against the disease and other reasons.[3]
Given the multiple uncertainties about the Bexsero meningococcal B vaccine product, I question why the Therapeutic Goods Administration allowed this vaccine product to be registered in the first place?
The TGA is funded by industry – is this an example of product evaluation failure by the conflicted regulator of vaccine products?
Despite the PBAC’s multiple rejections of the Bexsero vaccine, vaccine industry lobbyists continue to press for this questionable vaccine product to be added to the schedule, there are serious conflicts of interest impacting on vaccination policy.
In Australia it appears vested interests are trying to undermine the PBAC’s evaluation process by lobbying the States to implement mass meningococcal B vaccination programs, e.g. in South Australia.
Mr Marshall, I suggest you think carefully before implementing a novel vaccine program for a very rare disease, this is a serious matter that should not be a knee-jerk response to industry and media lobbying, particularly as this vaccine product is likely to be mandated if it gets onto the National Immunisation Program Schedule.
Is this about public health, or about developing lucrative vaccine product markets for companies such as GlaxoSmithKline?
Industry website FiercePharma reports that vaccines are a ‘financial bright spot’ for GlaxoSmithKline, with its ‘star’ Bexsero meningococcal B vaccine product having ‘stellar sales’.
GSK is building a US$175 million plant in Germany so it can expand production of the meningococcal B vaccine.[4]
Another FiercePharma report indicates GlaxoSmithKline is the vaccine industry leader with US$7.1 billion of vaccines sales in 2017, with sales for its meningitis vaccines (i.e. including Bexsero) growing 27% to US$1.24 billion.[5]
GlaxoSmithKline is developing a lucrative global market for its Bexsero meningococcal B vaccine, and it seems obliging governments are being persuaded to spend millions of taxpayers’ dollars on this questionable vaccine product for a rare disease, with Australia being at the forefront of this GSK campaign of questionable vaccine product for a rare disease.
A Sydney Morning Herald investigation into the health industry, published in 2010, revealed pharmaceutical companies are buying political access and influence through lobbying[6] – has GlaxoSmithKline ‘bought’ the South Australian government?
In South Australia the media has been used to fear-monger about meningococcal B to promote GlaxoSmithKline’s Bexsero vaccine trial involving 60,000 SA high school students, a vaccine trial that was supported by the former 4/5/2018 Gmail – Meningococcal B vaccination – conflicts of interest in vaccination policy Labor government.
In December 2016, The Advertiser reported “It is hoped the findings will provide a strong push to get the vaccine on the taxpayer-funded National Immunisation Program.”[7]
It seems this vaccine trial is biased from the outset.
It is alarming that a member of the Federal Government’s Australian Technical Advisory Group on Immunisation (ATAGI), A/Professor Helen Marshall, is the lead researcher on this GlaxoSmithKline-sponsored vaccine product trial, a serious conflict of interest.
While beating up the risks of meningococcal B in South Australia, A/Professor Marshall admits that meningococcal B is an ‘uncommon infection'[8], and yet promotes widespread mass vaccination of students with this still experimental vaccine product.
Do the students involved in this trial, and their parents, fully understand that the still experimental Bexsero vaccine was rejected three times by the PBAC, and that they are guinea pigs for this vaccine product for a rare disease?
Have they been sufficiently informed about the uncertainties of this product to properly give their ‘informed consent’ to participate in this industry-funded trial?
An advertisement currently being broadcast on television in South Australia coaxes students to continue their participation in this vaccine trial, saying “Help protect yourself, while also protecting your family and friends”. [9]
I suggest this advertisement is misleading as the long-term consequences of meningococcal B vaccination are unknown, which is the point of this unfortunately biased trial.
Again, it is alarming that a member of the Federal Government’s Australian Technical Advisory Group on Immunisation, A/Professor Helen Marshall, is leading this industry-funded vaccine trial.
According to the ATAGI conflict of interest document (see attached), A/Professor Marshall is an investigator on clinical trials associated with funding from GlaxoSmithKline, Merck, Novartis, Pfizer and Sanofi.
She also presents at conferences sponsored by vaccine companies.
Another ATAGI member, A/Professor Jodie McVernon, who was interviewed on Dr Norman Swan’s ABC Health Report discussing meningococcal B and W[10], is also an investigator on clinical trials funded by GlaxoSmithKline, bioCSL, Novartis and Pfizer, and is funded to attend workshops and symposiums sponsored by vaccine companies.
(These conflicts of interest were not disclosed when A/Professor McVernon was interviewed on Norman Swan’s ABC Health Report.
It is notable that in the interview with Dr Swan, A/Professor McVernon admitted meningococcal “is still a very, very rare disease”, and that meningococcal B has been “…slowly declining over time, for reasons we don’t understand”, i.e. before the implementation of meningococcal B vaccination.)
The former Chairperson of ATAGI, Professor Terry Nolan, also promotes the GSK Bexsero meningococcal B vaccine product[11], and along with A/Professor Helen Marshall and A/Professor Jodie McVernon, has been involved with meningococcal B vaccine studies sponsored by the vaccine industry[12].
Another avid promoter of the GSK Bexsero meningococcal B vaccine product is Professor Robert Booy, who is Head of Clinical Research at the National Centre for Immunisation Research & Surveillance, a government funded body which is influential on vaccination policy.
Professor Booy’s Clinical Research Group undertakes studies supported by vaccine manufacturers.
(The recently retired director of the NCIRS, Professor Peter McIntyre, was also an ex officio member of the Federal Government’s Australian Technical Advisory Group on Immunisation, and was also involved in industry-funded vaccine clinical trials – see the ATAGI conflict of interest document attached for some incomplete information in this regard.)
Professor Booy has lobbied for the Bexsero meningococcal B vaccine to be added to the taxpayer-funded national schedule, e.g. as reported in Medical Observer in August 2015 [13] and in the ABC News in November 2017[14].
Professor Booy is also a Board member and Chair of the Scientific Advisory Committee of the Immunisation Coalition, a vaccination lobby group which is sponsored and supported by GlaxoSmithKline, Pfizer, Sanofi Pasteur, Roche, Seqirus, Astra Zeneka, Mylan, and Bupa.[17]
Professor Booy’s association with the industry-sponsored Immunisation Coalition (formerly Influenza Specialist Group) was not disclosed in the Medical Observer article nor the ABC News report promoting the Bexsero meningococcal B vaccine, and is currently not disclosed on the Meningococcal Australia website, nor does it appear to be disclosed on the National Centre for Immunisation Research & Surveillance website. While Professor Booy and other academics are keen to flourish their academic affiliations, they are often reluctant to clearly disclose their associations with the vaccine industry.
It is wrong that members of groups and organisations influencing vaccination policy are also involved in industry-sponsored vaccine promotion and vaccine clinical trials, this is a serious conflict of interest.
The government should have independent specialists in infectious diseases to objectively consider the implementation of vaccination programs, not conflicted academics associated with the vaccine industry.
Note also that information on membership of ATAGI and conflicts of interest was previously shrouded in secrecy, and only came to light when citizens such as myself persisted in challenging then Federal Health Minister Nicola Roxon, and then Prime Minister Tony Abbott, for this information, see for example my letter to Tony Abbott dated 21 January 2015: http://users.on.net/~peter.hart/Letter_to_Tony_Abbott_PM_re_vax_policy.pdf
Similarly, the Immunisation Coalition/Influenza Specialist Group was reluctant to disclose the names of its members, this was only revealed after my persistent enquiries to the CEO, Kim Sampson.
Via industry-associated academics such as Helen Marshall, Robert Booy, Jodie McVernon, Peter McIntyre and Terry Nolan, the vaccine industry is influencing government vaccination policy, including government-mandated vaccination, e.g the Federal Government’s No Jab, No Pay law, and No Jab, No Play laws being implemented by some States.
Conflicts of interest are impacting on government-mandated vaccination policy, a serious matter in our liberal democracy where there must be transparency and accountability for vaccination policy.
Mr Marshall, the current Australian vaccination schedule for children is burgeoning with at least 46 doses of vaccines now being imposed on children via combination vaccine products and re-vaccinations.
I suggest children are being grossly over-vaccinated with this plethora of lucrative vaccine products.
There are emerging problems with vaccines, e.g. the pertussis/whooping cough vaccine, with acknowledgement from academia that “the startling global resurgence of pertussis, or whooping cough, in recent years can largely be attributed to the immunological failures of acellular vaccines…”[18]
It is important to consider if the implementation of a vaccine may result in unforeseen deleterious consquences, e.g. the emergence of new strains of disease, as Dr Norman Swan suggested on the ABC Health Report in regards to meningococcal, i.e. “Has immunisation caused the problem, in a sense?
In other words, that there is an ecological niche, if you like, for meningococcal infection.
You get rid of C because of immunisation, then B emerges, then C and W and Y, because there’s just an empty space for it to inhabit, a bit like sparrows…”[19]
The current over-use of vaccine products can be compared to the over-use of antibiotics, and also the over-use of other medical products such as opioids and anti-depressants.
We desperately need objective and independent specialists to consider the ‘big picture’ on the over-use of medical products, rather than academics conflicted by their associations with industry.
Mr Marshall, in regards to including the GSK Bexsero meningococcal B vaccination on the national schedule you have said “We will certainly encourage Greg Hunt to make sure those vaccines are available free of charge to children in SA under the age of two…If that isn’t forthcoming we will commit to making sure that the vaccine is available in SA”.[20]
Mr Marshall, on what do you base your commitment to “making sure the vaccine is available in SA”?
Mr Marshall, in light of the ‘multiple uncertainties’ about meningococcal B vaccination, and the conflicts of interest surrounding the promotion of the GlaxoSmithKline Bexsero meningococcal B vaccine product, I again ask you to very carefully consider the South Australian Government’s position on this matter.
Sincerely Elizabeth Hart
https://over-vaccination.net/
This email is being forwarded to Professor Andrew Wilson, Chair, PBAC; Mr Greg Hunt, Federal Health Minister; Stephen Wade, SA Minister for Health and Wellbeing; Mr Tony Pasin, Member for Barker; Mr Troy Bell, Member for Mount Gambier; and will also be publicly circulated to other parties.
References:
1. Meningococcal B victim Jordan Braddock’s family mount online awareness campaign. The Advertiser, 25 March 2018.
2. Vaccine push. The Border Watch (tbw.newsgroup), 29 March 2018.
3. See for example Recommendations made by the PBAC July 2015 – Subsequent decisions not to recommend.
4. GSK starts $175M plant to boost production of vaccine star Bexsero. FiercePharma, 22 March 2017.
5. GlaxoSmithKIine tops its peers with $7.16B in 2017 vaccine sales. FiercePharma, 13 February 2018.
6. The other drug war – the politics of big business. The Sydney Morning Herald, 27 February 2010.
7. Free meningococcal B-strain vaccine for 60,000 SA high school students under study into immunisation effect. The Advertiser, 13 December 2016.
8. Statements made in video included with the online article Meningococcal B victim Jordan Braddock’s family mount online awareness campaign. The Advertiser, 25 March 2018.
9. B Part of IT | TVC – 30 secs, video currently accessible on Youtube.
10. The segment titled ‘Deadly meningococcal W concerns’ included discussion on meningococcal B. ABC Health Report, 30 January 2017.
11. Meningococcal B vaccine: why aren’t we using it more? MJA Insight, 6 November 2017.
12. See for example: Perrett KP et al. Immune responses to a recombinant, four-component, meningococcal serogroup B vaccine (4CMenB) in adolescents: a phase III, randomized, multicentre, lot-to-lot consistency study.
Vaccine. 2015 Sep 22;33(39):5217-24; Terry Nolan et al. Vaccination with a multicomponent meningococcal B vaccine in prevention of disease in adolescents and young adults. Vaccine 33 (2015) 4437-4445; Terry Nolan et al. Persistence of Bactericidal Activity at 4 Years After 2 Primary Doses of a Recombinant, 4-Component, Meningococcal Serogroup B Vaccine (4CMenB) and Response to a Booster Dose in Adolescents and Young Adults. S322 OFID 2017:4 (Suppl 1) Poster Abstracts.
13. Meningococcal B vax rejection a bad move: expert. Medical Observer, 24 August, 2015.
14. Pressure grows to add meningococcal B strain to immunisation schedule, cases of disease rising. ABC News, 8 November 2017. In this article Professor Booy refers to the ‘effectiveness’ of the UK rollout of meningococcal B vaccination to justify implementation of the product in Australia. I await independent and objective evaluation of the Bexsero vaccine product in the UK. It is notable that Professor Booy failed to point out this vaccine product was also originally rejected in the UK, a decision that was overturned after intensive lobbying by vested interests, and when a person involved with the development of the Bexsero vaccine product, Professor Andrew Pollard, became Chair of the committee approving vaccine products, i.e. the UK Joint Committee on Vaccination and Immunisation, i.e. another example of conflicts of interest.
15. In December 2016 I emailed Professor Booy to ask if he or Meningococcal Australia received funding/support from the vaccine industry, but he did not respond. Subsequent to my email, the Meningococcal Australia ‘About’ page was updated to acknowledge receiving funding from GSK Australia and Pfizer Australia.
16. Subsidising meningococcal B vaccine deemed too costly for the federal budget. ABC News, 4 November 2016.
17. Immunisation Coalition ‘About us’, as downloaded 3 April 2018.
18. See for example Resurgence of Whooping Cough May Owe to Vaccine’s Inability to Prevent Infections which states “The startling global resurgence of pertussis, or whooping cough, in recent years can largely be attributed to the immunological failures of acellular vaccines”. A/Professor Christopher Gill says “This disease is back because we didn’t really understand how our immune defenses against whooping cough worked, and did not understand how the vaccines needed to work to prevent it. Instead we layered assumptions upon assumptions, and now find ourselves in the uncomfortable position of admitting that we…made some crucial errors. This is definitely not where we thought we’d be in 2017.” Boston University School of Public Health, 21 September 2017.
19. The segment titled ‘Deadly meningococcal W concerns’ included discussion on meningococcal B. ABC Health Report, 30 January 2017.
20. Demand for Steven Marshall to fund meningococcal B strain vaccinations program. The Advertiser, 20 March 2018.