
1. Robert Kennedy’s World Mercury Project: One in Nine Adverse Events Reported After DTaP Vaccination is Serious—But CDC Says, “Don’t Worry, Be Happy”
By The World Mercury Project Team – JULY 31, 2018
Until the 1990s, the vaccine administered to children for diphtheria, tetanus and pertussis protection was the DTP vaccine, one of the first combination vaccines ever licensed by the U.S. Food and Drug Administration (FDA).
However, as a “whole-cell” vaccine (meaning that it contained the entire Bordetella pertussis organism rather than purified components), DTP had a significant downside—including published safety concerns dating back to the 1930s and widespread reports of neurological damage emanating from both the United States and other countries.
By 1991, the Institute of Medicine cautiously reported that the evidence was “consistent with a possible causal relation between DTP vaccine and acute encephalopathy” [brain disease].
To pacify a concerned public, the Centers for Disease Control and Prevention (CDC) advised a phase-out of the whole-cell vaccine around 1991, while promoting an “acellular” version called DTaP (diphtheria, tetanus and acellular pertussis).
By 1997, the switch had taken place for all five doses in the series, recommended for infants and children at two, four, six and 15-18 months and 4-6 years.
In the two decades since the changeover, however, the DTaP vaccine has been plagued by embarrassingly low effectiveness.
A 2018 article characterized pertussis prevention as “an unresolved problem,” noting the “progressive increase” in pertussis incidence after introduction of the acellular vaccines and the need for ever more boosters.
Another recent commentary flatly stated that “pertussis is…not under control in any country” and that new types of pertussis vaccines are needed.
Nonetheless, on the safety front, health authorities have regularly praised the DTaP vaccines as offering a safer alternative than their whole-cell predecessors.
Is this reputation for safety well-deserved?
CDC researchers writing in June 2018 in Pediatrics seem to think so—but a closer reading of their findings suggests otherwise.
Examining DTaP’s track record
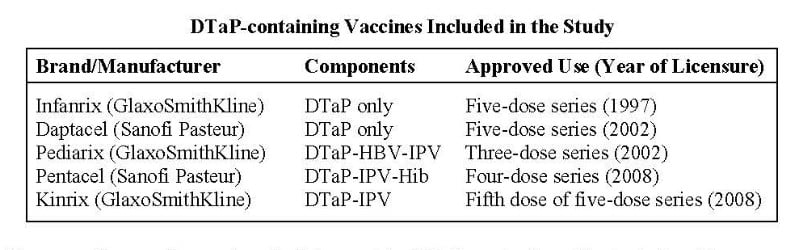
For their study, the CDC researchers assessed over two decades’ worth of data (1991–2016) from the CDC- and FDA-administered passive surveillance system called VAERS (Vaccine Adverse Events Reporting System), examining adverse events (AEs) reported to VAERS following vaccination with one of five currently licensed DTaP vaccines (see table).
The five vaccines included two DTaP-only vaccines (approved for the full five-dose series of shots) and three combination vaccines (approved for some portion of the DTaP series). The combination formulations in question included DTaP plus hepatitis B vaccine (HBV), inactivated polio vaccine (IPV) and/or Haemophilus influenzae type b (Hib) vaccine.
The researchers used several methods to consider DTaP vaccination risks, including
1) compiling all “serious” and “non-serious” adverse events reported to VAERS in association with the five vaccines over the designated time period;
2) clinically reviewing all deaths reported to VAERS following DTaP vaccination;
3) reviewing a subset (5%) of “non-death serious reports”; and
4) running an automated search of reported anaphylaxis following DTaP vaccination.
Not so safe
The analysis of VAERS reports identified tens of thousands of AEs (N=50,157) in the aftermath of a DTaP-containing vaccine.
(A single VAERS report may include more than one AE, so the adverse event categories are not mutually exclusive.)
VAERS, by the federal government’s own admission, captures only about 1% of AEs; thus, the 50,000-plus AEs probably vastly underrepresent the number of real-world DTaP-related vaccine injuries.
The study’s results illustrate the heavy burden of vaccines to which children in the U.S. are subjected.
For about 88% of the VAERS reports analyzed, children received the DTaP vaccine concurrently with one or more other vaccines, even though the five types of DTaP vaccine in and of themselves already constitute potent combinations.
Researchers who have looked at the number of vaccines administered at well-child visits have pointed out that American infants receive more vaccines in their first year than infants anywhere in the world.
Roughly one in nine (11.2%) of the reported AEs were coded as serious, and 15% of all serious AEs were deaths (844/5,627).
(If one were to average these deaths over the 26 years from 1991 through 2016, this would represent over 32 deaths annually.)
Of note, the investigators’ perusal of death certificates, autopsy reports and medical records showed that the reported cause for nearly half of the deaths (48.3%) was sudden infant death syndrome (SIDS), nearly always in children under six months of age.
Although the researchers dismiss the possibility of a causal relationship between vaccination and SIDS, evidence from other corners is strongly suggestive of just such a link.
In fact, it strains credulity to deny a plausible connection: many vaccines (including DTaP) are administered in bundles at health care visits around two and four months—exactly when nine out of ten SIDS deaths occur.
Serious but non-fatal AEs cited in 10% to 35% of all VAERS reports included systemic symptoms such as pyrexia (fever), vomiting, seizures/convulsions, diarrhea, lethargy and hypotonia (muscle weakness).
Anaphylaxis occurred far less frequently, but most reported anaphylactic reactions arose quickly—within 30 minutes of vaccination.
Seizures were the fourth most common serious AE reported.
Other studies have detected a heightened risk of febrile seizures when children receive DTaP simultaneously with other vaccines.
Febrile seizures are not benign (as once thought), which makes the frequency of post-DTaP seizures concerning.
The authors do not explain why they counted pyrexia as both a serious and nonserious AE, but it accounted for one in five of the latter.
As a potential sign of drug allergy and an indicator of a “systemic inflammatory response to a stimulus such as infection,” pyrexia and its prominence are noteworthy.
Back in 2004, other CDC researchers commented on the difficulty of ascertaining “the true importance of fever as an [adverse event following immunization]” and noted a lack of clarity regarding “how to interpret fever data derived from vaccine safety trials or immunization safety surveillance.”
What the study leaves out
Although the CDC authors noted that their analysis excluded Quadracel, the most recently approved combination DTaP-IPV vaccine (licensed in 2015), they curiously do not explain why they omitted several other licensed DTaP vaccines that were in widespread use during the time period in question:
- The Tripedia vaccine (manufactured by Connaught, which through a series of mergers became Aventis Pasteur and later Sanofi Pasteur) was approved as a fourth and fifth DTaP dose in 1992, 1996 and 2000; in 2001, Aventis Pasteur reformulated Tripedia and the FDA approved it for all five doses.
- Acel-Imune (manufactured by the now-defunct Lederle Laboratories) was approved for the fourth and fifth DTaP doses in 1991 and, in 1996, for the full five-dose series.
- The Certiva DTaP vaccine (made by North American Vaccine Inc., which was acquired in 2000 by Baxter International Inc.) was licensed in 1998 for doses one through five.
The authors also neglect to mention that all five DTaP vaccines included in their review contain one or more neurotoxic aluminum adjuvants, along with formaldehyde and polysorbate 80, a stabilizer for which information on potential chronic health effects is “not available.”
The Tripedia vaccine that the study excluded featured both aluminum and the mercury-containing preservative thimerosal.
Adverse events reported during post-approval use of Tripedia included “idiopathic thrombocytopenic purpura, SIDS, anaphylactic reaction, cellulitis, autism, convulsion/grand mal convulsion, encephalopathy, hypotonia, neuropathy, somnolence and apnea.”
By excluding these other acellular DTaP vaccines, the CDC study underestimates the magnitude of DTaP-related adverse reactions still further.
Weighing the risks
The CDC authors wrap up their assessment of DTaP vaccine safety with the boilerplate pronouncement that their analysis “did not identify any new or unexpected safety issues.”
Parents might disagree, wondering whether it makes sense to expose their child to a not-insignificant risk of serious DTaP-related injury when the risk of diphtheria is virtually non-existent in the U.S. (zero cases in 2016) and the risk of tetanus is likewise minuscule. (Tetanus, in any event, is non-communicable.)
Evaluating the risks of pertussis infection versus pertussis vaccination in different age groups is somewhat more complex but requires admitting up front that pertussis incidence has steadily increased (not decreased) in the U.S. since 1980, despite high vaccine coverage.
Discussing the problem of waning immunity, a 2012 study reported that “after the fifth dose of DTaP, the odds of acquiring pertussis increased by an average of 42% per year.”
In fact, the track record for whole-cell and acellular pertussis-containing vaccines shows that both are fraught with problems.
Back in 1993, researchers writing in the New England Journal of Medicine observed that a pertussis epidemic in Cincinnati had “occurred primarily among children who had been appropriately immunized” with the whole-cell vaccine. The same pattern of pertussis outbreaks in fully vaccinated populations has occurred with the acellular vaccines.
A related but underacknowledged problem is the role of vaccinated individuals as asymptomatic carriers and reservoirs of infection for vulnerable infants.
Finally, some researchers have suggested that pertussis vaccination may result “in selection of more virulent strains that are more efficiently transmitted by previously primed hosts.” Specifically, the acellular vaccines only contain B. pertussis antigens “that hold little or no efficacy against B. parapertussis,” which is another causative agent of pertussis infection; researchers concluded in 2010 that acellular vaccines “interfere with the optimal clearance of B. parapertussis” and may “create hosts more susceptible to B. parapertussis infection.”
Whether one focuses on safety or effectiveness, it is apparent that simplistic slogans and Pollyanna attitudes are no help in evaluating vaccine risks and benefits.
Ultimately, it should be up to parents—not CDC researchers biased against a fair consideration of risks—to make their own informed vaccine decisions.
2. Dr Judy Wilyman Report: Newsletter #205, Newsletter #206, Newsletter #207
Newsletter 205 – Medical Doctors and PhD Scientists Speak Out Against Vaccines
23 July 2018
The Australian government’s claims of safety and efficacy of vaccines are being underpinned by non-objective science provided by the pharmaceutical companies through industry-funded institutions and lobby groups.
Here is a link to the medical doctors and the PhD scientists who are providing the evidence of the harm that vaccines are causing in the population and the fact that doctors in Australia can no longer provide patients with these risks of vaccines for fear of being investigated by the government medical professional regulator (AHPRA).
The risks are being described as “anti-vaccination material” and health professionals can be de-registered for presenting this information.
This means doctors are breaching their Hippocratic oath to promote their patient’s best interest first – the Declaration of Geneva that is part of the Medical Board of Australia’s (MBA) good medical practice guidelines for doctors.
Instead doctors are being required by their regulations to promote the government’s schedule of 16 (~50 doses) vaccines to patients regardless of their individual genetics and without informing patients of the ingredients or serious risks of vaccines described by the Institute of Medicine (IOM).
Here is the link to 100’s of professionals warning you against vaccines – Medical Doctor’s and PhD Scientists Speak Out Against Vaccines.
I am listed at no. 72 on this list providing evidence of the harm coercive and mandatory vaccination policies are causing in populations.
This political situation is allowing unqualified people to promote false and misleading information about vaccines in the Australian mainstream media.
Human rights and health are being lost in Australia because:
- Politicians are being informed about vaccines by powerful industry/medical lobby groups with biased information and
- Non-qualified individuals from these lobby groups are permitted to use the official channels to suppress academic debate in Australia and to make fabricated complaints about professionals and academics who question vaccines to tarnish their reputations.
For evidence of the powerful lobby groups and COI in Australian vaccination policies, including the influence of Rupert Murdoch, please see below:
- Elizabeth Hart’s 30 min presentation demonstrating the COI of industry in government vaccination policies
- Elizabeth Hart’s letter to Rupert Murdoch and his influence in the No Jab No Pay/Play policies
- Judy Wilyman’s PhD completed at UOW (2015) that demonstrates the government’s vaccination policies are doing more harm than good in the Australian population
- Judy Wilyman’s 40 min presentation at the Censorship of the Vaccination Debate in Sydney (April 2018) describing why Australia’s vaccination policies are not “protective” public health policies and they are destroying the genetic fabric of the population (use the ‘not now’ button to view without signing into fb).
- My interview with Sarah Westall on Business Game Changers describing how global vaccination policies are being designed using non-objective science
- My webinar with the Australian Natural Practitioner’s Association (ANPA) titled ‘Informed Consent to Vaccination: Current Issues in Australia” that describes how the Nuremberg Code has been breached in the Australian No jab No Pay/Play legislation without the support of the Royal Australasian College of Physicians or the NHMRC in the Australian Immunisation Handbook (ED 10).
- Robert Kennedy Jr (attorney) recently used the freedom of information (FOI) act to request that the US Department of Health and Human Services (DHHS) show that it has fulfilled its duty to the public in providing safe vaccines since 1987.
Here is the document that proves that the US DHHS has failed to take any action over the last 32 years to ensure that childhood vaccines are safe.
This is relevant to Australia because we use vaccines that are licensed in the US and approved in Australia under a different name without further testing.
I have provided this information to the official Australian health authorities who deal with consumer complaints about health issues and I will provide you with their response when I receive it.
Newsletter 206 Health Minister Greg Hunt’s Comments on ‘Sacrificial Virgins’ are a Risk to Public Health
27 July 2018
The award winning documentary film exposing the dangers of the HPV vaccine titled ‘Sacrificial Virgins’ will be touring Australia this coming week starting on the Sunshine Coast Qld on 2 August.
Joan Shenton, investigative journalist says: “Sacrificial Virgins shows there’s no evidence that vaccines used in immunisation programs to guard against HPV will also prevent future onsets of cervical cancer – because there’s no scientific evidence that HPV actually causes such cancers.
However, the film provides plenty of evidence that, after vaccination, countless young women worldwide have experienced life-changing neurological damage.”
This vaccine was removed from the national immunisation programs in India and Japan in 2014 with many class actions occurring around the world.
Recently, in 2018 the worldwide debate of this vaccine was discussed in a Global Statement from Vaccine Victims from Five Countries.
But this is not discussed in the US or Australian mainstream media – this debate has been suppressed and censored in these countries as ‘anti-vaccination information’.
Australia’s Health Minister, Greg Hunt, has labelled the award winning film about the dangers of the HPV vaccine as making ‘dangerous and reckless’ claims.
He has made this statement without ever viewing the film and without finding out who the scientists are that he is criticising.
Our Federal Health Minister, Greg Hunt, is a risk to public health.
He does not have any health or scientific qualifications yet he is dismissing the claims made by reputable scientists in this award winning investigative film without any interest in seeing the film.
He simply states “I have no time for the false and reckless claims made by anti-vaxxers and I will continue to call out their dangerous claims.”
The Sydney Morning Herald article also states that immigration minister, Peter Dutton, has not ruled out banning this award winning investigative journalist from entering Australia for the tour.
In a similar way to the banning of Dr. Sherri Tenpenny, Polly Tommy and Ken Heckenlively who wanted to discuss the documented risks of vaccines that parents are observing and that are described in the medical literature.
This is a scientific issue and the public should be able to hear all the evidence for the multiple vaccines that have now been mandated for our children without the requirement for secret venues and the banning of speakers entering the country.
In 2011 I wrote a letter to Professor Fiona Stanley about the lack of proven efficacy, the harmful ingredients and the extremely high number of neurological reactions that were occurring to this vaccine.
She did not answer these questions and nor did the Therapeutic Goods Administration (TGA).
In 2013 scientists at the University of British Columbia picked up this letter and we had it published in the Infectious Agents and Cancer Journal.
In June 2013 my article titled “HPV vaccination programs have not been proven to be cost-effective in countries with comprehensive Pap screening and surgery” was published in the Infectious Agents and CancerJournal
https://infectagentscancer.biomedcentral.com/articles/10.1186/1750-9378-8-21
And presented at two international cancer conferences in San Francisco (2013) and London (2014).
At this time (2014) prominant leaders of the SAVN industry/medical lobby group David Hawkes and Dr. John Cunningham, who have influence with Liberal, Labor and Greens politicians (specifically Greens leader, Richard Di Natale) provided false information about the HPV vaccine to politicians.
The false information that they provided is described in Appendix 5 of my PhD thesis– Comment on the Hawkes et al 2013 Paper.
My critique shows that they have not supported their claims of safety and efficacy of the HPV vaccine, that they provided to politicians, with evidence.
In 2015 I presented a case study of the HPV vaccine in my PhD thesis – Chapter 9: Part 1 HPV and Cervical Cancer Pathoogenesis and Part 2 Undone Science in the HPV Vaccination Programs.
I summarised this researched information in an article titled ‘The Pharma Funded Promotion of HPV Vaccines”
In June 2018 my HPV vaccine research was put into a 20 min video presentation by LA Samer.
The video is titled “Gardasil/Cervarix HPV Vaccine – To Jab or Not to Jab?”
Now we have the award winning documentary ‘Sacrificial Virgins’ touring the east coast of Australia from 2nd – 13th August.
In the interests of your child’s heath and as someone who has studied the medical literature on this vaccine in-depth I highly recommend that you buy a ticket and investigate this unproven and unsafe vaccine.
The dates and cities that Sacrificial Virgins will be shown can be accessed from this link.
Newsletter 207 – Professor Fiona Stanley and the Australian Government have not Answered Questions on the HPV (Cervical Cancer) Vaccine
1 August 2018
In light of the news that the Australian government has not issued an entry visa to the award-winning investigative journalist, Joan Shenton, I would like to provide you with the questions on the HPV vaccine that were not answered by the Australian government and public health authorities in 2011 – four years after this vaccine had been used in Australia.
Many Australians are asking what the government has to hide by hindering medical practitioners (Dr. Sherri Tenpenny and Dr. Suzanne Humphries) and investigative journalists from coming to Australia to inform the public of the global debate on the serious adverse events to vaccines.
Please read the letter below that was sent to our Australian of the Year (2003), Professor Fiona Stanley, and to the Australian government regulator of vaccines – the Therapeutic Goods Administrator (TGA) – in 2011. These health authorities did not answer the questions that parents and researchers are asking about the safety and efficacy of vaccines:
This information was presented in the Infectious Agents and Cancer Journal in February 2013 and put into a 23 minute video by a pharmacist in June 2018
- This vaccine was not proven to be safe or effective against cervical cancer (CC) prior to its marketing in 2006.
Phase 3 trials were not completed until 2007.
In phase 3 trials this vaccine was only trialed for the prevention of pre-cancerous lesions in 16-26 year olds and not cervical cancer.
These lesions frequently clear quickly without treatment (in this age-group) and many never lead to cancer.
Therefore the vaccine is only assumed to be effective against CC because the relationship between pre-cancerous cells in young adults and cervical cancer 20 to 40 years later is still unknown. - Each of the 3 injections contains 225 ug of aluminium hydroxyphosphate sulfate, an adjuvant known to be linked with autoimmune diseases, the chronic illnesses that are increasingly common.
- Each of the 3 injections contains sodium borate (a pesticide), which has been linked to infertility, seizures and paralysis.
In 2005 the National Library of Medicine (NLM) of the National Institutes of Health declared this to be a dangerous poison and stated ‘it is no longer commonly found in medical preparations’.
HPV vaccine was approved in 2006. - Each of the 3 injections also contains polysorbate 80, an emulsifier linked with anaphylaxis, convulsions, collapse, seizure (twitching) and infertility in animals.
- Gardasil® has 3 times the number of adverse reactions reported as all other vaccines combined.
Since it was introduced, 94 deaths and 21,635 adverse reactions to Gardasil have been documented. Many have included the events listed above. - There is no systematic, long-term surveillance of adverse events to the HPV vaccine.
The reporting system is a passive surveillance system.
The CDC states “This (VAERS) data cannot be used to infer causal associations between vaccines and adverse events”.
If no one carefully monitors adverse reactions, there is no proof that it is safe. Yet parents are told combining vaccines is safe. This also means it will not be possible to determine whether women vaccinated against HPV will have a higher rate of infertility and autoimmune diseases in 10 – 15 years time. - The placebo in the clinical trials contained more aluminium adjuvant (a chemical linked with autoimmune diseases) than the vaccine itself. This casts doubt on the validity of the results.
Why has this vaccine been marketed so aggressively to Australian women when cervical cancer is a very low risk in Australia (indeed in all developed countries) and the vaccine contains chemicals linked with infertility? The other HPV vaccine (Cerverix) does not contain sodium borate or polysorbate 80, so why is it necessary to use infertility chemicals in Gardasil® which is being marketed to adolescent girls and women of all ages?
Yours Sincerely,
Judy Wilyman (2011)
My research on the HPV vaccine was published in cancer journals in 2013 and presented at international conferences but the Australian media would not report this research to the public. Murdoch owns approximately 80% of Australia’s media and here are his conflicts of interest in government vaccination policies.
The film the ‘Sacrificial Virgins’, that exposes the danger of HPV vaccines is showing on the east coast of Australia from 2 – 13 August 2018. Dates and locations for the events are listed here. In the interests of your children’s health please investigate what the Australian government is attempting to hide from the public by not providing a visa to professionals questioning vaccination.
Judy Wilyman PhD
Bachelor of Science, University of NSW
Diploma of Education (Science), University of Wollongong
Master of Science (Population Health), Faculty of Health Sciences, University of Wollongong.
PhD in The Science and Politics of the Australian Government’s Vaccination Program, UOW School of Humanities and Social Inquiry.
3. The Children’s Medical Safety Research Institute (CMSRI): Vaccine Boom, Population Bust – Study queries the link between HPV vaccine and soaring infertility
A plague is spreading silently across the globe. The young generation in America, the United Kingdom, France, Italy, Japan, Australia – in virtually every western country — is afflicted by rapidly increasing rates of infertility.
This spring, the United States reported its lowest birth rate in 30 years, despite an economic boom. Finland’s birth rate plummeted to a low not seen in 150 years.
Russian President Vladimir Putin recently introduced a string of reforms aimed at stemming the country’s “deep demographic declines.” The government of Denmark introduced an ad campaign to encourage couples to “Do it for Denmark” and conceive on vacations, and Poland produced a campaign urging its citizens to “breed like rabbits.”
The “population bomb” we were all endlessly warned about by environmentalists failed to blow, and instead, demographers have been trying to raise the alarm about the population implosion crisis unfolding across the West — the graying of societies facing an unprecedented aging demographic in which there will be too few young to support the old.
Most often, they blame social factors: young women embracing careers instead of motherhood, men shunning marriage and fatherhood, rising consumerism or couples choosing to delay raising a family until the economy settles.
But there is another phenomenon that is rarely mentioned – the growing numbers of young people who are not childless by choice but who are incapable of bearing children.

The Centers for Disease Control reports that more than 12 percent of American women – one in eight—have trouble conceiving and bearing a child.
Male fertility is plunging, too, and the trend is global.
Something – or things — are robbing young women and men of their capacity to procreate and public health admits it doesn’t have a clue where to start to fix the emerging priority.
Besides bantering about expanding access to costly and risky artificial reproductive technologies, very little is being done to discern the cause of the rising infertility crisis.
So, earlier this month, when an unprecedented study was released that looked at a database of more than eight million American women and singled out a whopping 25 percent increase in childlessness associated with one ubiquitous drug that young women have been taking for only a decade — in tandem with a marked decline in fecundity — you would have thought there would be significant interest from public health, the medical profession and the media, wouldn’t you?
A Common Denominator Behind Growing Infertility Rates
Instead, all three of these behemoths remain stone silent.
The reason?
Because the study, published in the current Journal of Toxicology and Environmental Health, examines the childbearing capacity of women who received the human papilloma virus (HPV) vaccine – compared to those who didn’t — and the results are chilling.
No one in public health, medicine or mainstream media, which are tangled up in the money-making machine of this vaccine, dare to publicly question the “safe and effective” mantra they’ve promulgated about Merck and GSK pharmaceuticals’ “blockbuster” commodity worth billions.
The study is by Gayle DeLong, associate professor of economics and finance, at Baruch College at City University of New York.
She observed that the declining birth rate had plunged in America in recent years – from 118 per 1,000 in 2007, to 105 in 2015 for the cohort aged 25 to 29.
The HPV vaccine was approved by the Food and Drug Administration for use in the US in 2006 to prevent cervical cancer – an illness women face a 0.6% lifetime risk of being diagnosed with.
Although it is diagnosed most frequently at age 47 in the United States, it was rolled out en masse, initially targeting girls aged 11 to 26 (and has since been marketed to boys as young as nine to prevent rare anal and penile cancers — a disease that afflicts 0.2 % of men in their lifetime.).
DeLong had read a case study in the British Medical Journal by Australian physicians Deirdre Little and Harvey Ward, who described a 16-year-old girl whose regular menstruation ceased after receiving HPV vaccinations and she was diagnosed with premature ovarian failure.
In 2014, the doctors published a case series of more teens who had entered premature menopause — a phenomenon Little and Ward described as ordinarily “so rare as to be also unknown.”
They raised troubling questions about some vaccine ingredients’ documented impact on reproduction, cited serious deficiencies (some would say criminal negligence) in preliminary vaccine trials and concluded that further research was “urgently required….for the purposes of population health and public vaccine confidence.”
As well, between 2006 and 2014, the Vaccine Adverse Event Reporting System (VAERS) cited 48 cases of ovarian damage associated with autoimmune reactions in HPV vaccine recipients. Between 2006 and May, 2018, VAERS catalogued other reproductive issues: spontaneous abortion (256 cases), amenorrhea (172 cases), and irregular menstruation (172 cases), all of which are likely under-reported symptoms.
All of this intrigued DeLong, who has followed the vaccine debate for years and makes no secret of the fact that she has two daughters, 18 and 21, both having been diagnosed on the autism spectrum, whom she saw regress developmentally and withdraw following vaccinations early in life.
“I am sceptical of vaccine science and the safety studies that are done, or not done,” she says.
She set out to analyze information gathered in the National Health and Nutrition Examination Survey (NHANES), which represented 8 million 25-to-29-year-old women living in the United States between 2007 and 2014.
Using logistic regression, she matched the young women for other variables, including age, and compared pregnancy as an outcome in those who received an HPV vaccine compared with those who did not get any of the shots.
“I just wanted to see if there was an issue,” says DeLong. “I certainly didn’t expect to find such a strong association.”
Approximately 60% of women who did not receive the HPV vaccine had been pregnant at least once compared to just 35% of women who had had an HPV shot had ever conceived.
For married women, the gap was also about 25%: 75% who did not receive the shot were found to have conceived, while only 50% who received the vaccine had ever been pregnant.
“Results suggest that females who received the HPV shot were less likely to have ever been pregnant than women in the same age group who did not receive the shot,” the study says.
It concludes, as all studies like this do, that the data points to an association, not causation, between the new vaccine and reduced fertility but that further study is warranted.
If the association is causation, however, DeLong’s math suggests that if all the females in this study had received the HPV vaccine, the number of women having ever conceived would have fallen by two million.
That’s not two million missing children.
That’s two million women who can’t conceive one, two, or any children.
It is millions of American children missing from a single cohort.
The implication, considering the sweeping breadth of the global HPV vaccine campaign targeted now at both males and females aged nine years old and up, is staggering.
The Skeptic Response
Skeptics are reliable vaccine industry defenders.
Armchair scientists who frequently hide behind pseudonyms, they have sort of schizophrenia about vaccines.
They insist vaccines are powerfully immune-modulating drugs capable of altering the immune system’s response to infectious exposure.
But they can’t accept that, like all drugs, vaccines can and do have thousands of documented long-term adverse reactions — especially because they are designed to induce the delayed manufacture of antibodies by the adaptive immune system.
Because these responses are mediated by the immune system, they are diverse, unpredictable and profound.
As expected, the Skeptics welcomed DeLong’s research with snide and personal (read unscientific) attacks.
They slammed her failure to include data on contraceptive use.
As a result, DeLong intends to attach that data to an addendum on the study, but what she found and reported on Age of Autism’s website only bolsters the study’s findings.
Among married women in the survey, 36.6 % of those who had received the HPV shot told the NHANES that they were using contraception (condoms at least half the time, birth control or injectables otherwise) compared to more than half (51.5%) of those who didn’t get the shot – a difference of almost 15%.
Less contraceptive use should translate to more babies among the vaccinated.
But, it seems that the vaccinated women in the study were actually trying harder to conceive (or at least not so worried about it) but still having less luck – not good for the Skeptic argument.
DeLong “isn’t even an epidemiologist” the Skeptics howled.
(In other words, shoot the messenger if you don’t like the message.)
To which she replies, “No. I’m not. I am a statistician, however. I would be grateful if epidemiologists would do their job and conduct this research thoroughly.”
This is precisely what her study called for.
If they did, mothers of vaccine injured children would not be required to.
Infertile Women Excluded From Study on Infertility
DeLong cites another study, from Boston University’s Schools of Public Health and Medicine and the Research Triangle Institute (RTI) in North Carolina, which found no such association between HPV vaccination and impaired fertility. Interestingly, Boston University has been the recipient of tens of millions from globalist vaccine promoters Bill and Melinda Gates Foundation, as has RTI, an organization that has received more than $47 million dollars in grant funds in recent years. RTI has published a number of recent studies on HPV vaccine, including one jointly-funded with GSK (a vaccine manufacturer) on the safety of the company’s HPV vaccine, and another, cautioning public health agencies to “take special measures to ensure their messages are not perceived as sponsored by drug companies” lest they incite “reduced liking and trust” by parents who will be less likely to give the HPV vaccine to their sons. Other RTI publications describe “Promising alternative settings for HPV vaccination of US adolescents,” changing “provider behavior” to enhance HPV uptake and more.
The RTI study about HPV vaccine’s impact on fertility was based on patients’ own recall of vaccines received (remember how the Skeptics howled at self-reporting before?).
But the study did not control for a far more important factor in fertility – age.
Age in this context affects not just the possible effect of the vaccine itself on fertility, but fertility is skewed dramatically in favor of the young and the study lumps 18 year-olds in with 30-year-olds.
As well, at the outset, it excludes 881 women from a pool of 5,020 because they were already trying – without luck – to conceive a baby for more than six months.
This has the effect of shrinking the infertility finding overall.
“These could be the women with ‘hard core’ issues of fecundity,” says DeLong, “but they are precisely the women who should be included.”
Environmental Concerns
To be sure, many environmental factors could be affecting female fertility.
Plunging male fertility is one of them. Male sperm counts have nosedived in recent decades – scientists published data last year showing that globally, they have dropped 50 percent in just the past 40 years – signalling serious unidentified environmental hazards.
Environmental scientists have pointed to everything from GMOs and toxic aluminum (more on this later) to Wi-Fiand birth control excreted by women into the drinking water, as possible causes of vanishing sperm and lowered fertility generally.
But in DeLong’s study, these environmental factors influence the whole group of women equally.
There is no reason why women who vaccinate would choose men with lower sperm counts, for example.
What’s in the HPV Vaccine?
So, what is it about a vaccine targeting a virus associated with cancer of the human reproductive tract that could go so wrong?
DeLong notes that both HPV vaccines contain aluminum, a toxic metal with documented potential to induce autoimmune self-attack, including on reproductive organs. HPV vaccines are loaded with aluminum: Merck’s original Gardasil vaccine contained 225 micrograms of nanoparticlized aluminum in each of three shots, totalling 675 micrograms; the “new improved” Gardasil 9 shots contain a total of 1500 micrograms – a wallop of stimulant for the immune system that DeLong thinks might just be “a tipping point” for youths who have had so many previous injections of aluminum in the schedule of 50 vaccines before school age.
Perhaps this is why HPV shots have such a high number of reported adverse events: 45,277 from its introduction in 2006 to May, 2018 (and these are considered to be vastly under-reported).
The CDC states that all these reactions are normal and that HPV vaccines are safe without any adverse impact on maternal or fetal outcome in pregnancy.
A recent paper from Texas Tech University Health Sciences Center cautions that this CDC assurance is based on incomplete data.
It points out biases in reporting and gaps in data.
“Certain adverse effects of the vaccine against HPV that have not been well studied as they are not well defined,” add the researchers who describe a host of documented, diverse autoimmune, neurological and cardiovascular disease in the wake of the vaccine.
The most frequent reported symptoms after HPV vaccination are poorly understood – fainting, chronic pain with tingling or burning sensations, headaches, fatigue, and dizziness, nausea and other symptoms that are worsened on standing upright, for example.
HPV vaccination – as well as tetanus vaccination – has been linked in medical literature to a condition called anti-phospholipid syndrome which is a poorly defined disease caused when the immune system erroneously manufactures antibodies against certain lipid proteins found in membranes that are in a host of tissues — eyes, heart, brain, nerves, skin – and the reproductive system.
One 2012 study by Serbian researchers at the Institute for Virology, Vaccines and Ser “Torlak” found that “hyperimmunisation” of the immune system with different adjuvants, including aluminum, in mice, resulted in induction of antiphospholipid syndrome and the tandem lowering of fertility.
Other research has implicated aluminum in conception problems.
French infertility researcher Jean-Philippe Klein and his colleagues at the University of Lyon published the results of their 2014 study of the sperm of men seeking assistance at a French infertility clinic.
They dispatched semen samples from 62 men who were having infertility issues to Christopher Exley’s aluminum research laboratory at Keele University in England where they were fluorescently stained to show the aluminum content as a luminescent blue.
“Unequivocal evidence” of high concentrations of the metal were found, especially in the semen of men with low sperm counts.
Clearly fluorescing and concentrated aluminum in the DNA-rich heads of the sperm led the researchers to speculate about what impact this may have on the ability to procreate and on the development of newly formed embryos.

The aluminum in DNA-rich sperm heads is stained blue by lumogallion.
Deirdre Little, the Australian GP who documented primary ovarian failure following HPV vaccination, has also criticized the fact that Merck’s product information was misleading about what sort of “saline” placebo was used in trials of the Gardasil vaccine – it failed to mention that the “placebos” contained both the high doses of aluminium as well as another scary ingredient, polysorbate 80.
This chemical has exhibited delayed ovarian toxicity to rat ovaries at all injected doses tested over a tenfold range.
None of the trials accurately assessed the long-term impact of the vaccine on the reproductive health of girls, Deirdre and Ward said, adding that drug damage to reproductive health may take years or decades to manifest.
Urgent and Unanswered Questions
The elephant in the room that no one wants to talk about is why the HPV vaccine is so heavily marketed to begin with?
Why make a vaccine for a disease that afflicts less than 0.3% of people in their lifetime?
And why include ingredients that are toxic, especially high doses of ingredients that scientists have objected to, and with documented toxicity to reproductive organs?
Why not use a true control in the trials?
What kind of scientist would do that kind of science?
What kind of public health agency brushes off 45,277 reports of adverse events – including neurological and reproductive symptoms — among young women of childbearing age?
Answering these questions turns out to be a lot more awkward than it seems at first.
There are chilling facts that are hard to set aside.
There are, as recently as 2015, the charges by Catholic bishops and human rights activists that public health agencies had deliberately tainted tetanus vaccines given only to women of reproductive age in Kenya.
Public health organizations denied they had laced tetanus vaccines with miscarriage-inducing Beta human chorionic gonadotropin (b-HCG) – a key sterilizing ingredient described in the extensive medical literature about the quest for a contraceptive vaccine to control population growth.
The Kenyan bishops insisted they had laboratory evidence that was ignored and the issue was ignored like DeLong’s study.
Another inconvenient truth is that the very people funding the HPV vaccine juggernaut are the same people most interested in reducing birth rates.
When Melinda Gates launched her Family Planning Summit in 2012 with the objective of bringing contraceptives to the world’s poor, it was clear she had one measure for that goal in mind: “If you see what’s happened in other countries that have had contraceptives, they use them first of all and the birth rates go down,” she said at the time.
“The question is could it have come down even more quickly?”
Although she swore her campaign was “not about population control,” Gates’ goals are the same as those who conducted the mass sterilizations of Indian men on railway platforms in the 70s and who continue to sterilize Indian women today en masse to get the birth rate down.
For Gates, success is not measured in access to clean water or energy or in the development of infrastructure or political freedom, it is measured in access to drugs, drugs she and her husband hold stock in: contraceptives and vaccines.
Their success is measured by exporting what most western countries are facing as social catastrophe: demographic decline.
So long as there is no satisfactory answer as to why the West is facing an infertility crisis, questions about the long-term impact of the HPV vaccine on human fertility are not only fair and reasonable, but the future is very bleak if we do not answer them.
One response to “The Safe Vaccine Debate – 1. Robert Kennedy’s World Mercury Project: One in Nine Adverse Events Reported After DTaP Vaccination is Serious—But CDC Says, “Don’t Worry, Be Happy” 2. Dr Judy Wilyman Report: Newsletter #205, Newsletter #206, Newsletter #207 3. The Children’s Medical Safety Research Institute (CMSRI): Vaccine Boom, Population Bust – Study queries the link between HPV vaccine and soaring infertility”
In Australia the Dtap vaccine (acellular pertussis vaccine) was not phased in until 1999-2004 (over a 4 year period). Prior to this we were using the whole cell pertussis vaccine and fully vaccinated communities in Australia (with 85-90% vaccination rates in infants) were still having ourbreaks of whooping cough through the 1990’s. There were 9 deaths in 1997-98 as vaccination rates were increasing and only 1 death per year for the previous 20 years before that.
Reference: Whooping Cough in Australia Research – https://vaccinationdecisions.net/wp-content/uploads/2011/09/Masters-Thesis-An-Analysis-of-the-Australian-Governments-Whooping-Cough-Policy-Policy-JWilyman.pdf