
1. NVIC : “Cookbook Medicine” and Mandatory Vaccination
The standardization of medical practice forces physicians to follow a script to achieve cost effectiveness and efficiency, but at what price to the patient?
Think about the last time you visited a medical office.
The nurse ushers you into the examination room.
He or she then proceeds to ask you questions from a checklist on a laptop while simultaneously typing in your responses.
The nurse barely makes eye contact with you.
After the checklist is completed, an algorithm in the computer generates a “to do” list based on your responses.
The physician enters the room, diagnoses your symptoms based on the computer algorithm, perhaps puts in a request for laboratory testing, writes a drug prescription for you and sends you on your way, all in a span of 10-15 minutes.
This process is known as “cookbook medicine”—a set of generalized clinical guidelines dictating how physicians should approach patient care.1

“Cookbook Medicine”: The Standardization of Medical Practice
Historically, physicians enjoyed professional autonomy in practicing medicine.2
They had the freedom to make informed decisions based on their own knowledge, expertise and judgment on what the best course of treatment was for each individual patient.
This personalized treatment used to be the norm in the practice of medicine and, as a result, the practice patterns of physicians varied from one another.2
In recent years, medical practice has undergone a metamorphosis.
In response to the variation of medical practice, the medical and health insurance industries have developed protocols and specific procedures to establish a “standard of care” that physicians are required to adhere to for all patients.3
There are several reasons for the streamlining of medical practice. In a report published in the Archives of Internal Medicine, the author Marshall B. Kapp, JD, MPH writes…
This push for formal explicit clinical standards emanates from a variety of sources for many purposes.
Third parties, both public and private, that pay for health care want to assure that the care they purchase on behalf of their beneficiaries is appropriate and efficacious.
Physicians, institutional administrators and other health care providers have a professional and ethical stake in assuring the quality of care.
Clinical standards may be used for such quality assurance purposes as licensure, privileging and other credentials review.
Additionally, the setting, dissemination and enforcement of clinical standards may be relevant for legal purposes, especially as evidence of fault or lack of fault in medical malpractice cases; this naturally attracts the interest of potential malpractice defendants and their insurers.”2
The standardization of medical practice forces physicians to follow a script to achieve cost effectiveness and efficiency, but at what price to the patient?
The Pitfalls of Streamlining Medical Practice
Focusing on efficiency may very well prove beneficial from a business perspective; however, there is a major problematic assumption underlying the standardization of medical practice.
The “cookbook medicine” approach operates on the false assumption that patients are not different from one another but simply belong to a homogeneous group and can all be viewed and treated the same way.
This “one-size-fits-all” approach results in missed symptoms and misdiagnosis, as well as unnecessary testing.4
It is estimated that “cookbook medicine” unnecessary testing contributes to $210 billion in additional health care costs.4 Hemal Kanzaria, MD, lead author of a study published in Academic Emergency Medicine states:
So many physicians acknowledged that they ordered tests for no medical reason, which makes it clear that physicians feel enormous pressure to behave in a way they may not want to.4
In an opinion piece published on the National College of Physicians website, one physician expresses his frustration with the standardization of medical care…
I wouldn’t do it again, and it has nothing to do with the money.
I get too little respect from patients, physician colleagues, and administrators, despite good clinical judgment, hard work, and compassion for my patients.
Working up patients in the ER these days involves shotgunning multiple unnecessary tests (everybody gets a CT!) despite the fact that we know they don’t need them, and being aware of the wastefulness of it all really sucks the love out of what you do.
I feel like a pawn in a moneymaking game for hospital administrators. There are so many other ways I could have made my living and been more fulfilled.
The sad part is we chose medicine because we thought it was worthwhile and noble, but from what I have seen in my short career, it is a charade.”5
Moreover, physicians are bound by contracts that are based on pay for performance, which usually means they must adhere to strict metrics, testing and treatment standards.6
According to an article in The New York Times authored by two physicians, Pamela Hartzband, MD and Jerome Groopman, MD:
For example, doctors are rewarded for keeping their patients’ cholesterol and blood pressure below certain target levels.
For some patients, this is good medicine, but for others the benefits may not outweigh the risks.
Treatment with drugs such as statins can cause significant side effects, including muscle pain and increased risk of diabetes.
Blood-pressure therapy to meet an imposed target may lead to increased falls and fractures in older patients.7
They further add that, “These measures are clearly designed to coerce physicians to comply with the metrics.
Thus doctors may feel pressured to withhold treatment that they feel is required or feel forced to recommend treatment whose risks may outweigh benefits.”7
Mandatory Vaccination Policies Mimic “Cookbook Medicine”
The principles of “cookbook medicine” are very evident in mandatory vaccination policies enforced in the United States and in other countries.
The U.S. Centers for Disease Control and Prevention’s (CDC) current vaccine schedules for children and adults take a “one-size fits all” approach and do not acknowledge an individual’s current state of health, personal or family health history, nutritional status and genetic predispositions prior to receiving vaccines.
Mandatory vaccination policies assume all human beings are part of a homogeneous group and do not have individual genetic, biological or environmental differences.
Arguments have been made that decisions regarding an individual’s vaccinations are not one-size fits all since exceptions to the schedule are sometimes made by doctors who have concluded there is a reason to delay or omit a vaccine to protect the person from being harmed by vaccination.
However, the truth is that the CDC and American Academy of Pediatrics (AAP) consider very few medical conditions as a reason to delay or omit a vaccination and 99.99 percent of children do not qualify for a medical vaccine exemption under narrow federal vaccine contraindication guidelines.8 9
The federally recommended and state mandated vaccine schedules do not factor in an individual’s susceptibility to vaccine adverse reactions, which the Institute of Medicine has pointed out cannot be predicted ahead of time by doctors, in part, due to gaps in vaccine safety.10
While “cookbook medicine” may serve a specific purpose for corporations and insurance companies operating health care systems, as well as for government health officials implementing “no exceptions” mandatory vaccination policies, this standard of care approach often fails to lead to better health outcomes for individuals.
2. Robert Kennedy’s World Mercury Project: Why Are the Same People Who Failed at Science on Agent Orange in Charge of Vaccine Safety and Developmental Disorders at the CDC?
By James Lyons-Weiler, Ph.D.
When historians write about the Vaccine Decades (1976–2020), there are two names that will live in infamy: Dr. Frank DeStefano, and Dr. Coleen Boyle.
In the 1980s, Congress mandated Agent Orange studies.
Frank and Coleen ended the studies two years early, insuring that “no link” would be found between illnesses being reported by injured veterans and dioxin.
The early termination of the study allowed the US Department of Veterans Affairs to deny any connection between Agent Orange and medical problems, preventing veterans and their families from qualifying for compensations.
Here’s your hurt, what’s your hurry. The Boyle/Destefano team bamboozle was outed by Admiral Zumwalt who went to the President and laid out the science in a classified report (now declassified):

“Without exception, the experts who reviewed the work of the Advisory Committee disagreed with its findings and further questioned the validity of the Advisory Committee’s review of studies on non — Hodgkin’s lymphomas .”
“a decision which should have been based on scientific data was reduced to vague impressions”
[One impartial review team’s results were] “a stunning indictment of the Advisory Committee’s scientific interpretation and policy judgments”
“1987 Followup Examination Results,” described statistically significant increases in health problems among Ranch Handers including all cancers”
“The work of the Veterans’ Advisory Committee on Environmental Hazards, as documented in their November 2, 1989 transcript, has little or no scientific merit, and should not serve as a basis for compensation or regulatory decisions of any sort.”
“the Air Force could just as easily have concluded that the health problems associated with the Ranch Handers were not necessarily related to eating beer nuts.”
“Shamefully, the deception, fraud and political interference that has characterized government sponsored studies on the health effects of exposure to Agent Orange and/or dioxin has not escaped studies ostensibly conducted by independent reviewers, a factor that has only further compounded the erroneous conclusions reached by the government.”
The Zumwalt report concluded:
 “It can, in my judgment, be concluded, with a very high degree of confidence, that it is at least as likely as not that the following are caused in humans by exposure to TCDD: non-Hodgkin’s lymphoma, chloracne and other skin disorders, lip cancer, bone cancer, soft tissue sarcoma, birth defects, skin cancer, lung cancer, porphyria cutanea tarda and other liver disorders, Hodgkin’s disease, hematopoietic diseases, multiple myeloma, neurological defects and auto-immune diseases and disorders.
“It can, in my judgment, be concluded, with a very high degree of confidence, that it is at least as likely as not that the following are caused in humans by exposure to TCDD: non-Hodgkin’s lymphoma, chloracne and other skin disorders, lip cancer, bone cancer, soft tissue sarcoma, birth defects, skin cancer, lung cancer, porphyria cutanea tarda and other liver disorders, Hodgkin’s disease, hematopoietic diseases, multiple myeloma, neurological defects and auto-immune diseases and disorders.
In addition, I am most comfortable in concluding that it is at least as likely as not that liver cancer, nasal/pharyngeal/esophageal cancers, leukemia, malignant melanoma, kidney cancer, testicular cancer, pancreatic cancer, stomach cancer, prostate cancer, colon cancer, brain cancer, psychosocial effects, and gastrointestinal disease are service– connected..”
President Clinton called Admiral Zumwalt “the conscience of the US Navy”. In fact, Zumwalt’s report is used by veterans seeking compensation. Zumwalt’s son was exposed to Agent Orange and died of lymphoma in 1988.
Boyle and Destefano’s Role in Agent Orange Pseudoscience
The CDC study (which lists no authors) that was published did not study any specific mechanism by which Agent Orange might have caused health issues in veterans. Instead, it studied dioxin levels in Vietnam veterans compared to non-Vietnam veterans. The 646 Vietnam veterans studied by CDC who all served in units that were most likely exposed, did not have elevated levels of dioxin as compared to non-Vietnam veterans. This retrospective study seeking differences of levels of dioxin nearly two decades after exposure is a type of epidemiologic study with only a long shot at success. The aims of the study were to determine whether military records could be “used to identify US Army Vietnam veterans who were likely to be exposed to the herbicide Agent Orange”.
Dioxin is stored in fat. The study measured dioxin levels in serum. Given the CDC’s failure to detect evidence for increased exposed in the 1980s, the ill-posed study was initially used as justification for no further science on the possible effects of exposure.
The analysis and conclusions were also blasted by a Congressional Report:
Human Resources and Intergovernmental Relations Subcommittee, US House of Representatives: The Agent Orange Cover-up: A Case of Flawed Science and Political Manipulation. 101st Congress, 2d Session, House Report №101–672. Washington, DC: Govt Printing Office, 1990.
What else has the Destefano/Boyle team failed to detect?
Under their watch, studies conducted ostensibly to test the hypothesis of a link between vaccines and autism have consistently failed to detect any association.
Are they competent enough, given the debacle of their failed study in 1988, to run the hopefully entitled “Immunization Safety Office” (which ignores the differences between Vaccination and Immunization) and the “National Center on Birth Defects and Developmental Disabilities”?
It is my professional opinion that no, neither of these individuals is sufficiently competent to be involved in vaccine safety science and interpretation of studies.
Further, it is my professional opinion that both are guilty of intentional and scientific fraud, perpetuated repeatedly and consistently, to hide the association between vaccines and neurodevelopmental disorders.
(1) Boyle informed Congress that no studies have been conducted that compares the rates of autism in vaccinated and unvaccinated Americans. Yet the CDC website clearly reads “Vaccines Do Not Cause Autism”. How could any competent scientist make such as stunning conclusion when the science required to answer the question has not been conducted?

Dr. Coleen Boyle testified to Congress that no science exists that shows vaccines do not cause autism, yet the CDC website still proclaims that “Vaccines Do Not Cause Autism”.(2) Destefano removed results showing increased risk of autism from on-time MMR prior to presenting to the Institutes of Medicine, and prior to publishing the fraudulent study known as “Destefano et al., 2004”. Two subgroups are missing: African American boys, and isolated autism. The latter group had increased risk, included boys and girls from any race, who had no other conditions other than autism. That means “anyone”.

Dr. William Thompson confessed his role in allowing false reports to be published both in audio recordings to Dr. Brian Hooker, and in statements from his lawyers. He was put on leave after reporting his concerns to then CDC Director Julie Gerberding, who put him on suspension for breaking rank. Dr. Walter Orenstein is also implicated in the cover-ups. See vaxxedthemovie.com and youtube.com/watch?v=hlxdWfTLHH0(3)
Boyle personally attempted to reconfigure the study design of that same study in an attempt to make the association of on-time MMR and autism go away. The team played with study design after knowing the increased risk of autism had been found, which is not allowed in objective research.
They worked very hard to attempt to make the association go away.
They play games with birth certificates, and age-group definitions.
Nothing worked.
So they simply removed the results:
(4) DeStefano admitted to journalist Sharyl Attkisson that (a) they removed the results because they did not believe them, and (b) that vaccines may be responsible for autism in susceptible individuals (See Sharyl Attkisson’s capture and hear the confession to her here).
 Dr. Frank DeStefano’s career exemplifies a list of failures to detect anything wrong with vaccines.
Dr. Frank DeStefano’s career exemplifies a list of failures to detect anything wrong with vaccines.
“I guess, that, that is a possibility,” said DeStefano. “It’s hard to predict who those children might be, but certainly, individual cases can be studied to look at those possibilities.”
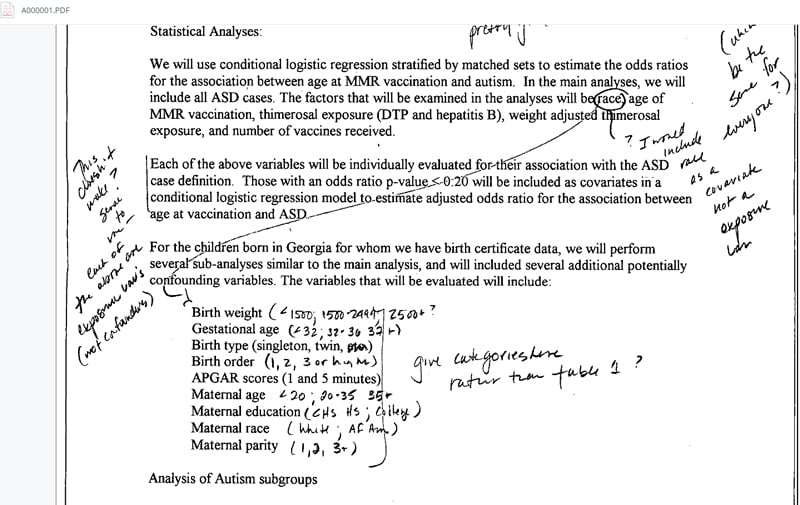
(5) DeStefano has participated in other publications in which he outlines how association studies should be conducted. He says that covariates must be “corrected for”, and that finding covariates that cause associations between vaccination and adverse events to disappear after the association is first found and then lost due to such corrections somehow exonerates vaccines. This is poppycock. If birthweight, mother’s age, mother’s income, gestational age, etc. cause a loss of significance of vaccination status, the correct model selection procedure is to look for interactions between vaccines and the covariates — especially because they can be functionally related to adverse events from vaccines. If the interaction terms are significant (which could easily be, given that mother’s income, age, gestational age and birthweight may all correlate to nutritional status), the result is pointing to covariates that make vaccination an increased risk. This is elementary linear modeling, and any studies that “correct for” covariates without also studying, and reporting, the interaction terms is hiding the effects of vaccines interacting with other variables.
Given these realities, and the fact that this and other equally damning information has been available for at least three years, it simply is unconscionable that Destefano and Boyle remain in their positions at the CDC. We cannot have incompetent individuals unable to conduct and properly interpret science standing in the way of helping America deal with the explosion of neurodevelopmental disorders — and the full suite of consequences currently being experienced in schools and homes all around the country.
Cowardice at CDC is Not Leadership with Accountability
These people are not only incompetent. They are cowards. Here, we learn from Dr. Thompson that Coleen Boyle refused to ever testify to Congress again.
CDC abdicated its responsibility to accountability for their policies:
(recorded May 24, 2014) Page 25 —
Dr. Thompson: Well let me tell you something really interesting I learned about this week so in the midst of this. Ya know, I was yelling at Marshalyn this week, I mean, Marshalyn and I were . . . WHOOOO! I was, it was suggested I resign, and um it’s like that type of stuff going on right now. The whole place is a big pressure cooker . . . So I don’t know if you know this. The CDC was invited to testify (before Congress) and they declined, so this is . . .
Dr. Hooker: Really?
Dr. Thompson: Yeah, and Marshalyn said she’s been offered to testify and said she won’t. Coleen (Boyle) said she’s been offered to testify and Coleen said that she would never go and testify again.
May 20, 2014 — the hearing which Thompson is talking about and Boyle and CDC declined to attend:
Examining the Federal Response to Autism Spectrum Disorders (5/20/2014)
The rate of ASDs is now 1 in 36. Frank, Coleen, you can stop the denialism. It’s over. And you can help America. How? Please resign, and in your letters of resignation, provide a full confession, like Dr. William Thompson has, and let someone capable try to clean up the mess you’ve made.
Vaccines can cause autism in some people, and, from the looks of things, in many people, and you know it. You failed to adjust the schedule, or offer meaningful public health advice in terms of vaccine safety. Your deeds are having profound effects on society, which are difficult to grasp:
- Half of children have a mental illness in the US.
- Teachers cannot teach children due to behavioral anomalies.
- Violence in schools are causing special education teachers to quit in schools across the country.
- Property taxes are going up as special education costs skyrocket.
- Calm rooms are being built in schools, and wobble chairs to allow fidgeting.
- Rates of schizophrenia are increasing among 20–30 year olds.
- High levels of amyloid are found in the brains of kids with severe autism.
- High levels of aluminum are found in people with autism.
- Artificial immunization programs are failing as parents abandon them due to first-hand experience with neurological and immunological adverse events.
- Exemptions to vaccine mandates are increasingly under fire.
There are desperate attempts ongoing now to convince the increasingly vaccine injured public that vaccine injuries are rare, to blame ASD on stress in the home, and most recently on alcohol use during pregnancy. Why now, all of sudden, can such association be detected? Where were these studies of environmental exposures conducted by CDC after 1988?
There were none. CDC (i.e., Boyle, Destefano) had a suspicious lack of curiosity of what DID cause autism. CDC convinced IOM to say that no more studies were needed.
Sound familiar?
CDC failed to detect association, and called for no more science. Just like Agent Orange.
Studies of genetics have revealed 850 genes associated with autism, but no single gene explains more than 1% of ASD. No studies have looked for genetic/vaccine interactions — and they must be conducted to fill in the gap. “No studies” does not mean “negative evidence.” It means “we need more science.”
The future is now. Vaccines can no longer be said to be “safe” and effective. Other science has progressed, independent of CDC, and the cat is out of the bag.
History will recall the names Destefano, Boyle, Orenstein, Gerberding — and Thompson. There are others. History has shown us that propaganda has never been successful in propping up a regime founded on fraud.
It’s time for Vaccine Safety Science Reform at the CDC, and across the United States.
First we need competence.
About the author: James Lyons-Weiler is the president and CEO of the Institute for Pure and Applied Knowledge, an advocacy group that pushes for accuracy and integrity in science and for biomedical researchers to put people’s health before profits. An established academic and researcher, he has a bachelor’s degree in biology, a master’s degree in zoology, a PhD in ecology, evolution, and conservation biology, and a postdoctoral in computational molecular biology; and he’s the author of Ebola: An Evolving Story and Cures vs. Profits.
3. The Dr Judy Wilyman Report: Newsletter #192 – Informed Consent to Vaccination is being Removed based on Industry Funded Studies
Newsletter 192 Informed Consent to Vaccination is being Removed based on Industry Funded Studies
27 February 2018
The Australian and US government’s support for mandatory and coercive vaccination policies – a medical intervention for healthy people – is a civil or criminal offence that violates constitutional rights and bodily integrity. Yet the Turnbull government is enforcing these policies for 16 vaccines based on industry-funded research.
There is no independent research on vaccines being used in government vaccination policies.
Industry-funded science is not objective science and it is being promoted by powerful industry-funded lobby groups in Australia through the media and in government vaccine advisory boards through representatives with financial conflicts of interest with industry.
Many of the 16 vaccines listed on the national program were recommended whilst Terry Nolan was the chairman of ATAGI (2005-2014) – the vaccine advisory board that makes recommendations directly to the health minister and at the same time he was deputy chair of the NHMRC – the government body that decides the direction of government funding.
Here are some of the conflicts of interest with industry that Terry Nolan had during his decade advising the federal Health Minister.
In 2007 when I requested government funding for an independent investigation into childhood health outcomes and government vaccination policies my request was rejected.
In Australia comedians and journalists are being used to stigmatise professionals and parents who have researchd this topic, as ‘anti-vaxxers’ – as if you shouldn’t discuss the risks of a medical intervention.
If the government had the science it would not be necessary to use comedians and journalists to prevent scrutiny of the medical literature by bullying.
Did you know that governments do not use improvements in children’s health as the measure of the success of vaccination programs? They use vaccination coverage as the measure of success.
They no longer use infant mortality rates because since 1995 these rates have shown that the countries using the least vaccines (Sweden and Japan) have the lowest childhood mortality (death) and morbidity (chronic illness) rates.
Sweden has also stated it will not adopt mandatory and coercive vaccination because of the serious health risks associated with vaccines and the violation of constitutional rights.
And did you know that vaccines did not reduce the risk of infectious diseases in the community? Public health reforms reduced this risk by 1950 in Australia.
This is why measles was not a disease to be feared and there was no vaccine in Australia until 1969 – and then it was voluntary.
These are myths (lies) perpetuated by governments using industry-funded science because governments are guaranteeing a market for the many vaccines that pharmaceutical companies are manufacturing.
And there are many more vaccines to come and they want you vaccinated from birth to death.
Pharmaceutical companies are creating the chronic illness in the population with vaccines and then claiming they can make a vaccine to prevent these diseases.
These chronic illnesses are preventable but the government is running a $5 million propaganda campaign (an ‘education’ campaign would be based on objective scientific evidence) in the Australian media using comedians and journalists who are not informed of the other side of this scientific issue.
The Turnbull government has already removed people’s free choice in university courses, employment, social welfare benefits and early childhood education by linking these necessities to mandatory vaccination using 16 vaccines (no selective vaccination).
Here is an article on the dangers of the Hepatitis B vaccine that was linked to causing multiple sclerosis (an autoimmune disease) in the early 1990’s and the lack of benefit or necessity for giving this vaccine to newborn infants.
Industry is using epidemiological studies to manipulate study outcomes and to confuse the public on the cause of many of these illnesses. Doctor’s are claiming the illnesses to be a ‘coincidence’ after vaccination and informing patients they do not know the cause of these diseases. But you will find that these chronic illnesses (in particular autoimmune diseases) have been listed on the industry package inserts for decades.
Then of course we have our federal Health Minister, Greg Hunt, claiming vaccines don’t cause autism. This is another myth (lie) perpetuated by govenrments so they can continue making billions from the vaccine industry.
Vaccines do cause autism and the rate of autism is increasing exponentially each year. This is a tragedy and it is a civil offence or crime for any government to remove informed consent without coercion to medical interventions.
Australia needs comedians and journalists that will do their jobs properly and report on the public interest in this medical procedure – the risks of vaccination.
Currently we are getting bullying and propaganda from journalists and comedians in Australia – which supports the industry’s interest in these policies.
Dr. Judy Wilyman
Bachelor of Science, University of NSW
Diploma of Education (Science), University of Wollongong
Master of Science (Population Health), Faculty of Health Sciences, University of Wollongong.
PhD in The Science and Politics of the Australian Government’s Vaccination Program, UOW School of Social Science, Media and Communication (re-named the School of Humanities and Social Inquiry in 2014).